Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
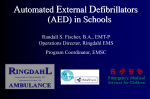
Myocardial infarction wikipedia , lookup
Jatene procedure wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
LAY RESCUER (OR HEART SAVER) BASIC LIFE SUPPORT TRAINING REFERENCE FOR SUN RUN LEADERS IF A PATIENT HAS ANY LIFE -THREATENING ILLNESSES OR INJURIES CALL AN AMBULANCE! BY: RON STRAIGHT ALS PARAMEDIC, MEd CanROC EMS Liaison/Coordinator TABLE OF CONTENTS Objectives Definitions Cardiovascular Disease Risk Factors for Cardiovascular Disease Medical Problems attributed to Cardiovascular Disease Signs and Symptoms of Stroke, Heart Attacks and Angina Chain of Survival Patient Positioning Serious Bleeding Control Airway Obstructions A) Conscious Patient (*adult and child ) Partial Airway Obstruction B) Conscious Patient with a Complete Airway Obstruction C) Conscious airway obstructed collapses unconscious – one rescuer D) Unconscious Patient with a complete airway obstruction E) Noticeably pregnant or very obese patients that are obstructed. F) Conscious infant obstructed (less than 1-year-old) G) Conscious to unconscious or unconscious infant is obstructed (<1 year) Cardio Pulmonary Resuscitation and AED provision (CPR/AED) A) CPR – Adult & Child B) CPR – Infant (<1 yr.) C) Non-breathing Adult, Child or Infant D) AED – Adult (>8 years of age or 2o sexual characteristics) & Child (1-8 yrs.) E) Defibrillation/AED application Terminology: Advanced Cardiac Life Support procedures Barrier Devices Cardiac Arrest Research Chest Compressions with no Ventilating Defibrillation Hypothermia Life-threatening or “deadly” bleeding Mouth to Nose Oxygen Therapy Regurgitation Re-position the patient if required. Signs of revival Sudden Cardiac Arrest followed by dying gasps References 3 3 4 4 4 5 5 5 5 6 6 6 6 7 7 7 7 8 10 10 11 11 12 13 13 13 13 13 13 14 14 14 14 14 15 15 15 16 2 OBJECTIVES: 1. 2. 3. 4. 5. 6. Describe the purpose of and actions for providing Basic Cardiac Life Support. Demonstrate Basic Cardiac Life Support procedures for all age groups. Describe the cardiovascular risk factors and methods of prevention. Describe and demonstrate the use of an AED. Describe and demonstrate the management of heart attack, angina and stroke patients. Define all the items listed under terminology. DEFINITIONS: automatic external defibrillator American Heart Association major blood vessel leaving the heart normally full of oxygen rich blood. The coronary arteries branch off this vessel and run back to supply the myocardium When the heart is no longer able to propel enough blood into the vessels to keep the Cardiac Arrest person responsive (awake), breathing normally or showing other signs of adequate circulation. lay rescuers define a child as 1 – 8 years of age. Health care providers define a Child child from age one up to the development of secondary sexual characteristics (i.e. facial hair in men, breasts in women). Coronary arteries vessels that supply the heart its own blood supply primary muscle of breathing below the lungs Diaphragm Electrocardiogram a picture of the electrical activity of nervous conduction through the heart. (ECG) Normally each deflection above or below the isoelectric (base) line is labeled by a progressive letter starting with the letter ‘P’. Emergency Medical Services EMS the ‘food pipe’ or tube from the mouth to the stomach. Esophagus a person employed and trained to provide CPR/AED at a higher level. Health Care Provider (HCP) rescuer’s hand closest to the patient’s head Higher hand death of tissue due to no blood supply usually from a blockage of a vessel Infarction general public, a person whose position does not necessitate the provision of Lay rescuer (LR) CPR/AED at a higher level. rescuer’s hand closest to the patient’s feet Lower hand heart muscle Myocardium heart attack or blockage of a vessel feeding an area of the heart Myocardial Infarction (MI) breastbone Sternum blowing in a breath of air or delivering oxygen to the lungs Ventilation AED AHA Aorta 3 CARDIOVASCULAR DISEASE Cardio refers to the heart and vascular refers to the vessels. Disease is a disorder or ailment. Cardiovascular disease can impair blood circulation to parts of the body, especially the brain and heart. This is due to blockage or damage to blood vessels. The arteries that give the heart its own supply of blood are called the coronary arteries. Atherosclerosis is the build up of plaque in arteries that can restrict blood flow or dislodge and cause blockages. RISK FACTORS FOR CARDIOVASCULAR DISEASE Controlling or avoiding these factors reduce your risk. The following acronym may assist you in remembering these factors: (You can change these*) How Come Some Die How Many Shall Live On And Recover high blood pressure (>120/80)* cholesterol that’s too high (triglycerides, LDL)* smoking is #1 risk factor* diabetes or family history of heredity, history of heart disease in the family males are more prone until women reach menopause stress is too high* lack of exercise* overweight* age over 40 race MEDICAL PROBLEMS ATTRIBUTED TO CARDIOVASCULAR DISEASE Stroke: when blood supply to part of the brain is stopped due to a ruptured or blocked blood vessel Angina Pectoris (pain in the chest): a narrowing of a coronary artery resulting in less blood reaching the heart muscle. It is a medical condition most often caused by a build up of plaque on the walls of the artery. Patients are usually prescribed nitroglycerin which dilates arteries, improves blood flow through the coronary arteries and lessens the work load on the heart. Heart Attack (myocardial infarction or MI): when part of the heart muscle does not receive blood usually from a blockage of a coronary artery. This can result in death of the affected area unless measures are taken, usually in-hospital, to renew circulation. This can be accomplished by clot-busting drugs (thrombolytic therapy); balloon-inflated widening of the affected artery (angioplasty); fixed tube placement in the affected artery to hold it open (a stent); or surgical rerouting by putting a bypass vessel around the affected area. The success of these treatments is time-dependent. If the blockage is to a significant vessel(s), the heart can stop pumping blood effectively and go into cardiac arrest. STEMI: if a person suffers a heart attack (MI) it can be indicated by a change in their ECG (see diagram below). If there is an elevation in the ST section it is called an ST elevation MI or STEMI. If these patients can be transported (by ambulance) to a hospital capable of inserting a stent (In the ‘CATH Lab’ – a catheter or tube is run up a blood vessel into the heart to place the stent [mesh metal tube] into the affected vessel to open it up) within 90 minutes from the onset of the attack, the area supplied can be saved. Cardiac Arrest: when the heart is not beating effectively and not enough blood is being pumped to create a palpable pulse and circulation cannot be found. Brain damage can occur in 4-6 minutes without a blood supply. CPR can prevent the onset of brain damage. 4 A normal picture of one heart beat on an electrocardiogram. Each deflection is labeled by a letter. If you look at the area between the S and T wave you can see it is elevated. This can be an indication of a recent heart attack. SIGNS AND SYMPTOMS OF: Stroke –headache (worse than before); visual problems; unable to speak or difficulty speaking; weak or limp on one side of the body; unresponsive. Assess the person by having them perform the following to look for deficits: (1) smile – compare sides (2) speak – slurring (3) hold out arms with eyes closed – arm drifting down or can’t raise one. Heart attack and Angina –chest pain that may spread to arms, back, neck & jaw; feeling short of breath; pale; sweating; nausea; vomiting (these three more often point to a possible MI); denial. With angina, nitroglycerine is usually prescribed. It most often comes as a spray to administer under the tongue. It is usually administered every 5 minutes usually up to three times. If symptoms persist after 3 nitro (5 minutes apart) or pain or symptoms are different than usual angina pain, it is possible that the person is having a heart attack (MI). As many as one third of first-time men and half of first-time women had unrecognized symptoms with their MI (Framingham study). Half of these had no symptoms at all. Diabetics and women may present with fatigue or less significant symptoms. CHAIN OF SURVIVAL™ A chain of factors to consider for the prevention and care of cardiovascular disease. The links are: healthy choices early recognition - early access - early CPR - early defibrillation - early advanced care - early rehabilitation. Each is a link to survival with the chain being as strong as its weakest link. PATIENT POSITIONING If the patient is dizzy or light headed lay the person down to permit circulation to the brain. If the person feels short of breath, sit them up to allow easier chest expansion. If the person is unresponsive, lay them on their side so their tongue does not block their airway and anything in their upper airway/mouth can drain out or can be removed. SERIOUS BLEEDING CONTROL The body holds ~5 litres of blood. Bleeding is potentially life threatening when an artery is spurting blood or a third of the blood volume has been lost (7+ cups). To control bleeding, if possible, elevate the bleeding part above the heart, apply direct pressure and sit or lie the person down. If blood soaks through a dressing apply another over top. (It should be noted that there has been no research to show that elevation stops or reduces bleeding so AHA 5 have stated they can no longer endorse the use of elevation, just direct pressure. Practical experience informs all paramedics to continue using elevation prior to application of direct pressure.) AIRWAY OBSTRUCTIONS (THE “A” IN CIRCULATION–AIRWAY – BREATHING – DEFIBRILLATION) A) A CONSCIOUS PATIENT (ADULT AND CHILD ) WITH A PARTIAL AIRWAY OBSTRUCTION 1. The patient can speak or cough and has some air exchange. Some air can move through the trachea or windpipe. The patient coughing is the most effective procedure for freeing a partial obstruction. If the patient is upright, have the patient lean forward and encourage the patient to cough. If the patient starts to turn blue and is about to collapse because of a lack of air (oxygen) then treat like a complete airway obstruction. B) A CONSCIOUS PATIENT WITH A COMPLETE AIRWAY OBSTRUCTION 1. When asking the patient if they are choking, they confirm and are unable to speak and maybe cough weakly. They cannot say anything. The patient may grasp their throat and look very anxious. 2. Abdominal thrusts are delivered by the rescuer compressing the lungs to force the obstruction up and out of the airway. The rescuer stands behind the victim, reaches around with one arm placing their fist, thumb first, against the abdomen, just above the navel and well below the breastbone. The rescuer’s other hand reaches around and grasps on top of the fist. 3. The rescuer thrusts (pulls) in and up repeatedly until the obstruction clears in the conscious patient or the patient collapses. “Until it pops or they drop.” This technique puts pressure against the diaphragm and, in turn, the lungs. 4. If the patient is on their back on the ground refer to C9 & C10 but do not attempt to inspect, clear or ventilate unless unresponsive. 5. If abdominal thrusts don’t work on an upright patient, consider trying chest thrusts (see pregnancy). or back blows (hit with the flat or your hand between the patient’s shoulder blades to loosen the object to be coughed out). It had been cited in the international findings that retrospective research indicates that airways obstructions have most often been cleared with a combination of all three techniques. C) A CONSCIOUS AIRWAY OBSTRUCTED PATIENT WHO COLLAPSES UNCONSCIOUS – SINGLE RESCUER 1. Try to prevent patients from injuring themselves by trying to slow their fall and protect their head. 2. Call the ambulance service (911). If the patient is unresponsive the ambulance must be called immediately or call a code if in the hospital. Delegate someone to call and report back to you to be sure. If you are alone with the victim, quickly leave to first call 911 if the cause of the collapse could be cardiac otherwise work for 2 minutes to correct the problem (obstruction) before leaving to quickly call. 3. Kneeling beside the patient’s chest, landmark on the chest to perform chest compressions. The rescuer exposes the chest, places the heel of one hand between the patient’s nipples on the breastbone, the other hand is placed on top, and the fingers are interlocked. With a child (between 1 and 8 years of age) compress the chest with one or two hands 4. The single rescuer now begins 30 compressions at a rate of 100/min. Compress the chest at least 2 inches down, or, with a child, at least 1/3 of the way down. The arms are locked at the elbow so straight arms are pushing straight down using the weight of the upper body. This rhythmical, pistonlike motion should ensure that the hands do not leave the chest between compressions but that the rescuer allows full chest expansion (comes all the way back up). The count is 1..and..2..and.. 3.. up to 30. 6 5. Look in the person’s mouth. Only if seen, try and hook the object out by sliding down the inside of the cheek, way down to the back of the throat If two rescuers, the second rescuer can visualize the mouth to clear any foreign bodies. 6. Airway – Open it using the head tilt / angle of the jaw lift. Place the rescuer’s higher hand on the patient’s forehead to tip the head back. Open the person’s airway by lifting under the angle of the patient’s jaw with the fingers of the rescuer’s lower hand. 7. Ventilate – The rescuer, while tipping the head back, pinches the nose and seals their mouth around the patient’s mouth and blows in two slow 1-second breaths allowing air to escape between each one. The lower jaw is held up continually. Do not blow in if the patient is breathing out. Use a barrier device between you and the patient, if available. Each breath blown in should be given slowly over 1 second to produce visible chest rise so air won’t go down the esophagus and enter the stomach causing the patient to regurgitate. 8. If no air goes in, reposition the head (tip it back further) to ensure the airway is open and try to ventilate again. 9. If still obstructed, repeat C3 – C8 until the airway is cleared and the patient can be ventilated or the patient starts breathing. 10. Once the airway is open, does the patient start to move, breathe effectively, cough? If not, check for circulation (5 – 10 seconds), looking for movement and normal breathing. Normal breathing is when the patient takes a breath at least every 6 seconds. If no circulation start compressions followed by ventilations at a 30:2 ration if one or two rescuers. You are now performing CPR to provide artificial circulation. 11. If no response, go to CPR A6 (see page 10) D) AN UNCONSCIOUS PATIENT WITH A COMPLETE AIRWAY OBSTRUCTION (UNKNOWN UNTIL DETECTED) 1. See CPR A (page 10) except inspect the mouth after each set of 30 compressions before you ventilate. If at any time when compressing to clear the airway, should something appear in the mouth, clear it out. E) NOTICEABLY PREGNANT OR VERY OBESE PATIENTS THAT ARE OBSTRUCTED. The rescuer may not be able to effectively provide abdominal thrusts to an upright or sitting patient with a large abdomen. The rescuer does not want to potentially harm a pregnant woman’s foetus. To unobstruct these patients, chest thrusts are provided instead of abdominal thrusts. If the patient is erect, from behind, reach around under the arms and landmark your fist on the middle of the breastbone and thrust inward until the airway clears or the patient collapses. If unable to apply or if ineffective, back blows can be applied (B5 above). If the patient is on the ground treat them as any patient (see C and D above). F) CONSCIOUS INFANT OBSTRUCTED (LESS THAN 1 YEAR OLD). To confirm an obstruction, assess to see the infant is not breathing. The chest may be tugging in and out. There is no crying. Infants become cyanotic (blue) very quickly when without oxygen. Invert the infant and support upside down face down with the bottom arm and hand holding the infant’s head against your thigh when in a sitting position. Give 5 back blows or slaps between the shoulder blades. Sandwich the infant between both arms, supporting the head and roll the infant face up on the other thigh. Give 5 chest thrusts with two fingers placed one finger width below the line between the nipples. Depress the chest 1/3 the way down. Repeat until the infant either becomes unconscious or unobstructs (likely cries). 7 G) CONSCIOUS TO UNCONSCIOUS OR UNCONSCIOUS INFANT IS OBSTRUCTED (LESS THAN 1 YEAR OLD). Refer to CPR Infant (page 10) except look in the mouth and clear foreign material after each set of compressions or should it been seen. CARDIO PULMONARY RESUSCITATION AND AED PROVISION (CPR/AED) The purpose of CPR is to deliver oxygen rich blood to the arrested heart and the brain (and body) via chest compressions and ventilations. It is achieved by blowing in air (oxygen) and then pushing on the chest to circulate the oxygen from the chest to the body. It has now been found that it takes upwards of 10 effective compressions before the heart and brain begin to be perfused (supplied) with blood. Only after ~10 compressions each time was some perfusion provided. For all age groups, cycles of 30 compressions followed by two 1-second breaths is repeated. It is felt that even short stoppages in compressions can be fatal (more than 10 seconds). Chest compressions should be provided smoothly and rhythmically. Insure that each compression is at the appropriate depth and that the rescuer allows full recoil of the chest on the upstroke (unweighting). This mechanism better permits blood to enter the chest (on the up-stroke) and then be delivered to the heart and brain (compressions of appropriate depth and timing [100/min.]). When a person suffers a cardiac arrest, the heart stops providing effective blood flow. The heart is made up of four chambers or pumps, two (left and right) atria and two ventricles. Oxygen depleted blood from 8 the body returns to the right atrium, which in turn pumps the blood to the right ventricle. The right ventricle pumps the blood up to the lungs to rid the carbon dioxide and renew its supply of oxygen. The left atrium receives the oxygen rich blood and delivers it to the left ventricle, which pumps it to the body through the aorta. The coronary artery leaves the aorta and branches to feed the heart muscle (myocardium) with its own oxygen supply. The nervous system of the heart is initiated by an automatic pacemaker called the sinoatrial node located at the top of the right atrium (see diagram below). It is called the pacemaker because it sends out impulses faster (60-80x/min) than other areas of the heart’s nervous system. These impulses progressively travel down through the heart’s nervous conduction system stimulating muscle cells to contract (see diagram below). Blood is pumped out of the top chambers into the bottom chambers then out of the heart (to the lungs and body). When the heart’s own blood supply is interrupted or stopped by a blockage in a coronary artery (heart attack or myocardial infarction), the area affected can start to send out impulses very rapidly overriding the pacemaker. If this occurs in the ventricles its can result in a fibrillating (quivering) or very rapid beating heart that can’t provide blood flow. These abnormal rhythms or arrhythmias are called ventricular fibrillation and pulseless ventricular tachycardia. These uncontrolled rapid arrhythmias can be corrected with a shock or defibrillation. Cardiac arrests can also result from a motionless heart called asystole (flat line where no electrical activity occurs) or pulseless electrical activity or PEA (where usually the heart is getting minimal or ineffective nervous stimulation). These arrhythmias have little chance of conversion and are therefore often fatal. PEA can also occur with blood loss and the heart attempts to circulate blood (normal contraction) with no effect. Neither of these rhythms benefit from defibrillation. It must also be appreciated that nervous conduction problems can also happen in the atria (upper chambers). This may result in other abnormal heart rhythms or arrhythmias. These higher-up arrhythmias are usually able to effect circulation and blood flow. Do not let names like atrial fibrillation and atrial tachycardia mislead you, since these are not ventricular in origin. These are rarely sudden causes of collapse and cardiac arrest. Since they cause the heart to work harder, they may eventually lead to an MI or a heart attack and in turn a cardiac arrest. With a sudden cardiac arrest, initially, the abnormal heart rhythm (arrhythmia) is often ventricular fibrillation or ventricular tachycardia. To convert this a single defibrillation, only once every two minutes, is provided as long as the patient stays in this arrhythmia. Unless the patient was witnessed to 9 collapse and defibrillation occurred in the first minute, once a defibrillation is delivered it can take the weakened heart some time (minutes) before it can provide effective perfusion or blood flow. Therefore, after a defibrillation, compressions are started immediately. Only if the patient shows signs of return of circulation (movement, normal breathing, coughing, waking) does one stop. H) CPR – ADULT & CHILD (LAY RESCUERS DELINEATE A CHILD AS BEING 1-8 YRS OF AGE OR NOT HAVING ARMPIT HAIR OR BREAST DEVELOPMENT.) 1. Rescue scene evaluation. Check for hazards or dangers in the area. The rescuer must not put them self at risk for injury. 2. Assess Level of Consciousness. Ask the patient if they can hear you and pinch the top of the patient’s shoulders to see if they respond. 3. If not assess CAB – CIRCULATION-AIRWAY-BREATHING. Look for normal breathing for 5 – 10 seconds. If no response (no coughing, movement or normal breathing), presume the patient is in cardiac arrest. 4. Call the ambulance (911). If the patient is unresponsive, the ambulance must be called immediately. Delegate someone to call and report back to you to be sure. Ensure they understand you. If you are alone with an adult and the patient could have had a heart attack, quickly leave to call an ambulance and bring back a defibrillator if available. With a choking, drowning, an overdose or a child (with the cause not likely to be a heart attack), provide care for 2 minutes of CPR before leaving to call an ambulance since oxygenation not defibrillation is more likely required (for exceptions see K. below). 5. Landmark and compress the chest in the exact same manner as described when performing chest compressions to clear the airway of an unconscious patient (see C3 – C4 above). The only difference is that the purpose now is to provide artificial CIRCULATION because the heart is in arrest (not beating effectively). Through studies, it has been shown that even healthcare providers have difficulty finding a pulse and this has resulted in delays in providing compressions. Since compressions, if supplied needlessly, are not as deleterious as once thought, all lay (general public) rescuers are now encouraged to simply assess for circulation without a pulse check when deciding to start compressions. 6. The cycle of 30 compressions followed by 2 breaths is repeated until EMS (emergency medical services or an ambulance) arrives; you are relieved (every two minutes); you are too fatigued to continue; the patient shows signs of revival (a pulse, coughing, movement, normal breathing ); or it is too dangerous to continue. 7. A new compressor should take over every 2 minutes so fatigue will not affect the quality of compressions. 8. If an AED is available refer to D below. I) CPR – INFANT (<1 YR.) 1. Rescue scene evaluation. Check for hazards or dangers in the area. The rescuer must not put themselves at risk for injury. 2. Check level of consciousness. Yell at the infant for a response? If not... Pinch the top of the infant’s shoulder causing pain (do not move them if they may have hurt their neck), tickle the feet, and clap your hands. If the patient does not respond assume they are unresponsive. 6. CAB – CIRCULATION-AIRWAY-BREATHING. Assess for normal breathing (less than on breath every 3 seconds). If no response (abnormal breathing assessed for 5 – 10 sec.), call the ambulance (911). If the patient is unresponsive the ambulance must be called immediately. Delegate someone to call and report back to you to be sure. Ensure they understand you. If you are alone with an infant, perform 2 minutes of CPR before leaving to call an ambulance. 10 7. Landmark and compress the chest in the exact same manner as described when performing chest compressions to clear the airway of an unconscious infant (see G above). The only difference is that the purpose now is to provide artificial circulation because the heart is in arrest (not beating effectively). If the infant’s rate is less than 60 beats/min with signs of poor perfusion, even with oxygenation, start compressions. 8. The cycle of 30 compressions followed by 2 breaths is repeated until EMS or a code team arrives or you are relieved or too fatigued to continue or the patient shows signs of revival (coughing, movement, normal breathing), or it is too dangerous to continue. J) NON-BREATHING ADULTS, CHILDREN OR INFANTS WITH A PULSE. Ensuring that the pulse can be felt and CPR is not required, ventilate the adult one every 5-6 seconds, the child and infant every 3 seconds. If available and the patient is in shock or has been without oxygen, supplement breaths with oxygen. K) AED – ADULT, CHILD (NO SECONDARY SEXUAL CHARACTERISTICS). An automatic external defibrillator (AED) is a computer that automatically determines the type of arrhythmia (abnormal heart rhythm) and, if the arrhythmia could be corrected with a shock, it will charge up to defibrillate (shock) the heart. Once charged, semiautomatic defibrillators prompt the operator to push a button to shock. Automatic defibrillators, after charging and providing a warning, shock the patient automatically. The AED will automatically analyze, and shock if indicated, every 2 minutes. Ensure no one is touching the patient before the device defibrillates. An AED is most effective the sooner it is employed after a patient arrests. The arrhythmia a patient is in, after they collapse in cardiac arrest, is often ventricular fibrillation (VF) or ventricular tachycardia (VT). With time this arrhythmia can change into a less viable rhythm that an AED will not defibrillate. The arrhythmias that cannot be helped with a defibrillation are not a displaying rapid electrical activity like VF or VT. These less chaotic arrhythmias are electrical mechanical dissociation (electrical activity that does not result in cardiac output) or asystole (a flat-line). The chances of revival with these arrhythmias are generally poor. It is hoped that good CPR will change these arrhythmias into ones that can be shocked. If the patient has been down in cardiac arrest for too long (~10+ minutes with no CPR), the patient will have little if any electrical activity left in the heart. Then the AED will not shock. The patient’s chances of revival are poor. The conditions that are most likely to result in a shockable rhythm are heart conditions or electrocution. Cardiac arrest as a result of drowning, drug overdose, allergic reactions, suffocation or trauma are more likely to result in a rhythm that is not shockable. The focus on these patients is effective CPR with oxygenation. If a child collapses suddenly from a blow to the chest from a small high speed object like a baseball or hockey puck, if the child has a history of heart problems or if the child was electrocuted, consider applying an AED (even if only adult pads are available.) Two minutes of CPR are first performed and if there are no signs of circulation, apply and follow the AED prompts. With a small child or infant, if pads will touch when applied on the front, apply them front and back over the lower sternum. Initially, if the adult does not respond and there are not signs of life or normal breathing (a breath every 5 seconds or more), then initiate CPR and apply the AED pads as directed on and by the device (AED). Follow the prompts. Whether the AED delivers a shock or not, if the adult is in arrest, immediately continue providing CPR for 2 minutes. The analysis/shock and two minutes of CPR will be repeated until the patient shows signs of revival or other emergency personnel relieve you. It is 11 unlikely a person in cardiac arrest can be resuscitated after 30 minutes of effective CPR and AED provision. If the pads won’t stick (hairy chest or wet) correct the problem (shave or if extra pads - remove pads with hair and apply other pads, or dry the chest). If the patient is in standing water (not just wet ground), move to dry land. If it is wet between the pads (e.g. rain), dry between the pads so the shock, if delivered, won’t travel over top of the chest, through the water, using the path of least resistance. Most AED’s have disposable razors with them. L) DEFIBRILLATION – AED APPLICATION: 1.Turn the AED on by pushing the button or opening the lid. Lay it down beside the patient. The AED will direct you through steps. 2.Expose the chest as needed to attach the pads to the chest (upper right – just below the collar bone and lower left - below and to the side of the nipple). If the patient had a medication patch, remove it. If the patient has a pacemaker or implantable defibrillator under the skin, do not apply the pads over the device. If the patient’s chest is wet, dry it. If the patient has a hairy chest, shave where the pads will adhere. 3.Do not touch the patient (other than carefully checking the pulse, if appropriate) as the AED automatically analyzes the heart rhythm since movement can affect its analysis. 4.If the AED charges, once charged, ensure no one is touching the patient and push the shock button immediately. Not defibrillating immediately can reduce the effectiveness of a defibrillation. 5.Immediately resume CPR until the AED analyzes again, you are relieved or the patient begins to breath and you find a pulse. Diagram on the front of one make of an AED showing pad placement with the AED on the ground beside the patient’s head. Rescuer would be prompted to push red button if AED determined a shock was required. 12 TERMINOLOGY BARRIER DEVICES – Lay Resecuers should use a barrier device if ventilating a patient. These can be as simple as a plastic shield with a one-way valve to prevent patient air, fluids and vomit from contacting the rescuer. Another more effective, acceptable device are ventilation masks or “pocket-mask”. Whatever the device is employed, the rescuer(s) should be practiced and proficient in its use. Maintaining a seal is necessary to deliver air into the patient (ventilate). The rescuer should maintain this seal as they deliver each ventilation. It is appreciated that 80% of cardiac arrests happen in the home and without a barrier device, providing mouth-to-mouth may be necessary to the friend or relative. CARDIAC ARREST RESEARCH – The Resuscitation Outcomes Consortium (ROC) is a consortium of physicians, paramedics and nurses undertaking research on the provision of pre-hospital cardiac arrest and trauma care. It was realized that immediate defibrillation after an arrest is the most effective. If an arrested person was not witnessed to arrest by the first responding EMS crew, immediate defibrillation has not been found to be as effective. The coarseness or significance of ventricular fibrillation (degree of shaking or amplitude) is known to decrease with time without blood flow to the heart. This is due to the heart muscle running out of oxygen. If a heart is defibrillated when not oxygenated and in a ‘fine’ ventricular fibrillation, the heart likely will not convert into a perfusing rhythm that will create circulation. It is more likely to deteriorate into asystole or a pulseless electrical rhythm, both that have a poor prognosis for recovery. If the heart is re-oxygenated, by performing effective CPR for a period of time, prior to the first defibrillation, the heart is more likely to be defibrillated into a perfusing rhythm. A recent ROC study, that compared participants performing CPR for 30 seconds as compared with 3 minutes prior to the first analysis and potential defibrillation, showed both methods were equally effective. Therefore compressions should be administered for 30 seconds before defibrillation with patients who have been in arrest without CPR for more than 4 minutes. ROC is continuing to conduct in the field (pre-hospital) cardiac arrest trials. The trials currently being conducted at 10 sites/cities by pre-hospital providers in Canada and the US are: o Non-stop compressions with interposed breaths vs 30:2 CPR o An ani-arhythmic drug comparison for patients in VFib cardiac arrest. Amiodorone vs Lidocaine vs a placebo. This is to determine if these drugs improve survival to discharge. CHEST COMPRESSIONS WITH NO VENTILATING – If you are unwilling to ventilate, at least provide compressions. If the patient suddenly collapsed without oxygen depletion, simply circulating the blood for the first few minutes is effective. This advice is given to 911 callers who describe a sudden collapse indicative of a VFib or VTach arrest. In BC they are advised to push 600 times and by then the ambulance should have arrived. If the person drowned or suffocated and had run out of oxygen before their heart has stopped, then compressions alone without added ventilations would circulate blood without oxygen. DEFIBRILLATION An electrical shock from a machine called a defibrillator is what is critical for the revival of a patient in cardiac arrest. For every minute that passes without CPR there is a 7-10% less chance of survival with patients in ventricular fibrillation or v. tachycardia. Approximately 30% of all cardiac arrest patients are in this rhythm. The remainder have less chance of revival. With effective CPR there is a 4x greater chance the defibrillation will be effective. 13 CPR provides, at best, 30% of normal blood circulation and allows the rescuer added time for successful defibrillator use. After 10 minutes without CPR, the chances of recovery are slim. If the patient has been in arrest for more than four minutes, it is now believed that there is value in “priming” the heart or performing CPR for a period of time (30 seconds) before defibrillating. This provides needed oxygenation to the heart and increases the chance that a defibrillation will convert the arrhythmia into an effective rhythm. Stopping compressions, too shallow, too few or not allowing the chest to rise all the way up between compressions results in poor circulation to the heart and brain. Automatic External Defibrillators (AED’s) are programmed to shock only once at a time every two minutes if the heart is in a rhythm that will benefit from a shock. If the heart stops due to a lack of oxygen to the body (like suffocation or drowning), and is not due to a heart-related illness, then CPR, alone, may revive the patient if started soon after the arrest. In these cases there may be no heart damage. Only half of cardiac arrests occurring in a public place are in a rhythm that can be defibrillated, so it should not be surprising that the AED says, “No shock advised.” Continue CPR and the AED will reanalyze every two minutes. HYPOTHERMIA has been found to prolong the time that a patient may survive a cardiac arrest. If a person is found cold and possibly hypothermic and has no signs of circulation, start CPR. The saying is, “They are not dead until they are warm and dead.” LIFE-THREATENING OR “DEADLY” BLEEDING – The adult body holds approximately 5 litres of blood or ~21 cups. The child or infant holds proportionately less. Most bleeding is not severe and can be managed routinely with elevation and pressure. If there is a wound to an artery (vessel leaving the heart), it is under pressure and is likely to spurt blood quickly. This can be “life-threatening” if not stopped. If the blood is not spurting (vein or capillary) but the patient has lost one third or more (> 7 cups) this also is treated as life-threatening. Stop the bleeding immediately. This is best achieved by applying direct pressure on the wound with a bandage or cloth. If it soaks through, do not remove but apply another on top. Sit or lay the patient down. If no bones are broken and movement won’t cause further injury, elevate the part above the heart to aid in slowing the flow of blood. MOUTH TO NOSE - Closing the mouth and blowing in the nose is an acceptable alternative if the patient’s mouth won’t open, is injured or the rescuer would prefer to blow in the patient’s nose. OXYGEN THERAPY Supplemental oxygen can be important. Appreciating that the air contains about 21% oxygen and our expired air still has 15%, a patient low in oxygen would benefit in the provision of additional oxygen. With a patient who is breathing and needs supplemental oxygen, with a simple inhalation mask, oxygen can be administered from a tank of compressed oxygen running in from a attached hose. With a patient who must be ventilated it should be run at 15 lpm. If applying a ventilation mask and the lay rescuer is blowing in the top, tubing is attached to a port so the oxygen accompanies the rescuer’s delivered breaths. The partial pressure of oxygen in the patient should be targeted at 94%. Over oxygenation can have deleterious effects in the post-arrest victim. REGURGITATION – If the patient has vomit in their airway at any time due to the techniques you employ (ventilations, chest thrusts, analyzing with an AED, defibrillation), if performing compressions and by yourself, finish the cycle to 30 then turn the patient to clear the airway, ventilate the patient to ensure the airway is still clear and resume where you left off. If analyzing, if advised, deliver the shock then clear 14 the airway before ventilating. With two or more providers, compressions should continue while another provider clears the airway between ventilations. The patient is not breathing so the vomit will only enter the lungs if blown in. Stopping compressions, even for a few seconds can lesson the chances or recovery. So, with vomit, it is only necessary to clear out the mouth and upper airway before the patient is ventilated. RE-POSITION THE PATIENT IF REQUIRED. If the adult patient has vomit in their airway and they need to be turned to clear their airway or if the patient is breathing and has a pulse and must be left, place the patient in a drainage or recovery position, on their side. It is not recommended to position young children and infants on their side because the head positioning may result in airway occlusion (closing). With an arrested patient, simply turning the patient’s head with or without suction may also be effective for clearing the airway. Compressions can continue throughout with no immediate loss of blood flow to the brain and heart. If there may be a neck injury (unknown or unwitnessed patient found collapsed) or you suspect one and you must move the patient (unsafe scene or poor position), if possible, do so as a unit, supporting their head in relation to their body to minimize neck movement. If you cannot determine if the patient is breathing because of their position, carefully position the patient so you can. CAB assessment is most easily performed with the patient lying in a face-up position. Do not delay CPR. If CPR is required, the patient must be face up on a firm surface. Reposition the patient immediately. FORE AND AFT. If the patient must be moved: From behind, reach under the patient’s armpits (aft) and grasp their opposite wrists. Draw the patient to your chest so you are at the same height as the patient. Lift using your legs, not your back. Move the patient preferably with someone else lifting the legs (be‘fore’), to an appropriate position. SIGNS OF REVIVAL A sudden occurrence of the patient taking a breath may be a sign that the patient’s heart may have started beating. It may also just mean that the CPR performed has artificially stimulated the patient to breathe. It is acceptable to check the pulse when the AED is analyzing (as long as the patient is not moved). These brief pulse checks occur before defibrillation or after 2 minutes when compressors are changing. If there is not sign of life and there are no indications that a pulse may have returned, do not check needlessly, stopping compressions and stopping blood flow to the heart and brain. If a pulse is found, then check that breathing is adequate (adult 1/5sec., child 1/3-5 sec., infant 1/3 sec.) If breathing is not adequate, continue ventilating until breathing becomes regular at the appropriate rate. SUDDEN CARDIAC ARREST FOLLOWED BY DYING GASPS When someone first goes into cardiac arrest, the patient may first seizure from a lack of oxygen to the brain. There are many causes of a seizure and in this case, it will likely last less than a minute. The person may also make occasional, ineffective, “agonal” breaths due to residual nervous activity. This abnormal breathing can occur for a number of minutes. If the patient is not moving or coughing or showing any other signs of life, start CPR. These dying gasps actually may help pull blood into the chest as the chest expands, so more blood could be delivered when compressing. In cardiac arrest, the heart is not longer propelling blood effectively and CPR is essential. A study showed that agonal breaths increase the chances of survival. For examples, look on-line to YouTube http://www.youtube.com/watch?v=CBMxH4xtE8w or http://www.youtube.com/watch?v=ICODRFoWZkw&NR=1 15 REFERENCES Heart and Stroke Foundation of Canada 2015 Canadian resuscitation and first aid guidelines British Columbia Ambulance Service New 2006 CPR/AED Guidelines & Resuscitation Research Paramedic Manual Clark JJ, Larsen MP, Culley LL, Graves JR, Eisenberg MS: Incidence of agonal respirations in sudden cardiac arrest. Ann Emerg Med December 1991;21:1464-1467. ABOUT THE AUTHOR Masters Degree in Adult Education (UBC) 30+ years experience working as an Advanced Life Support Paramedic with the BC Ambulance Service in Vancouver attending to hundreds of cardiovascular emergencies. 35 years experience teaching and instructor-training in emergency cardiac care (BCLS & ACLS). Attended the first Resuscitation Fellowship in Seattle/King County 11/08. Seattle boasts the best save percentage of witnessed cardiac arrest in the field to discharge with normal neurological function (50% vs <10% in many large US cities. BC is 25%). EMS Liaison/ coordinator (BC representative) for frontier, a stroke study on the use of a new drug called NA-1, administered by paramedics, in hopes of preserving brain function until the patient arrives at hospital. EMS Liaison (BC representative) on the Canada Resuscitation Outcomes Consortium – the organization conducting research on pre-hospital cardiac arrests and trauma. Website: www.safelearning.ca Contact email: [email protected] 16