Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Dental degree wikipedia , lookup
Fluoride therapy wikipedia , lookup
Dental hygienist wikipedia , lookup
Focal infection theory wikipedia , lookup
Crown (dentistry) wikipedia , lookup
Oral cancer wikipedia , lookup
Special needs dentistry wikipedia , lookup
Remineralisation of teeth wikipedia , lookup
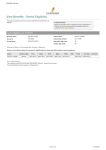
Guardian Anytime View Benefits - Dental Eligibility For faster processing, submit your claims electronically using Payer I.D. #64246 Predetermination When the expected cost of a proposed course of treatment is $300 or more, we recommend that a predetermination be submitted to the Claims Address. Dental Eligibility as of 03/02/2016 Member Name: TORREY, MATTHEW A Patient Name: TORREY, MATTHEW A Group ID: 00512404 Patient Date of Birth: 08/26/1976 Group Name: EQUIX, INC Dependent Age Limit: 26 Student Age Limit: 26 Effective Dates of Coverage (by Service Category) Below are the effective dates of coverage for eligible patients. Dates may differ between service categories. Name TORREY, MATTHEW A Relationship Prev Basic Perio Major Ortho Member 12/02/2015 12/02/2015 12/02/2015 12/02/2015 12/02/2015 TMJ Endo Oral Srg 12/02/2015 12/02/2015 Cosmetic Plan Information Your network is the DENTALGUARD PREFERRED DENTAL. Search for a Provider. Your benefit period is from January 1 to December 31. Page 1 of 3 03/02/2016 Guardian Anytime Coverage Information Coverage Information Preventive DentalGuard Preferred Dentist Deductible Waived DentalGuard Plus and Non Contracted Dentist Deductible Waived 100% Yes 100% Yes Last Eligible Service Cleaning/Prophylaxis THE PLAN COVERS EITHER ONE REGULAR PROPHYLAXIS OR A PERIODONTAL MAINTENANCE IN ANY 6 CONSECUTIVE MONTH PERIOD. Cleaning/Prophylaxis: Date Not Found Fluoride FLUORIDE IS COVERED UP TO AGE 19 SUBJECT TO ALL OTHER PLAN PROVISIONS. FLUORIDE IS COVERED ONCE IN ANY 6 CONSECUTIVE MONTH PERIOD. Fluoride: Date Not Found Oral Exams EXAMS ARE COVERED ONCE IN ANY 6 CONSECUTIVE MONTH PERIOD. Oral Exams: Date Not Found Palliative/Emergency Treatment Sealants SEALANTS ARE COVERED ON DEPENDENTS UNDER AGE 16. SEALANTS ARE LIMITED TO ONCE PER TOOTH IN ANY 36 CONSECUTIVE MONTH PERIOD. SEALANTS ARE COVERED ON PERMANENT UNRESTORED MOLAR TEETH ONLY. X-Rays BITEWING RADIOGRAPHIC IMAGES ARE LIMITED TO EITHER A MAXIMUM OF 4 FILMS OR A SET OF VERTICAL BITEWINGS, IN ONE VISIT, IN ANY 12 CONSECUTIVE MONTH PERIOD. FULL MOUTH SERIES OR PANORAMIC FILMS ARE COVERED ONCE IN ANY 60 CONSECUTIVE MONTH PERIOD. Other Preventive Services SPACE MAINTAINERS, RECEMENTATION OF SPACE MAINTAINERS AND HARMFUL HABIT APPLIANCES ARE CONSIDERED BASIC CATEGORY SERVICES. Basic Anesthesia 80% No 80% Bitewing: Date Not Found Full Mouth/Panoramic: Date Not Found No ANESTHESIA IS CONSIDERED WITH THREE OR MORE COVERED SIMPLE EXTRACTIONS OR ANY COVERED SURGICAL PROCEDURE. Consultation Endodontics/Root Canals Fillings (Amalgam/Silver, Composite/White or Tooth Colored) COMPOSITE RESTORATIONS ARE COVERED WITH NO SURFACE RESTRICTION. POSTERIOR RESINS (WHITE FILLINGS ON BACK TEETH) ARE NOT COVERED, AN ALTERNATE BENEFIT OF AN AMALGAM (SILVER FILLING) RESTORATION WILL BE CONSIDERED. REPLACEMENT OF EXISTING RESTORATIONS IS LIMITED TO ONCE IN ANY 12 CONSECUTIVE MONTHS FOR PATIENTS UNDER AGE 19, OR ONCE IN ANY 36 CONSECUTIVE MONTHS FOR PATIENTS AGE 19 AND OLDER. Oral Surgery ORAL SURGERY AND SURGICAL EXTRACTIONS ARE CONSIDERED MAJOR CATEGORY SERVICES. ORAL SURGERY CLAIMS FROM OUT OF NETWORK PROVIDERS SHOULD FIRST BE SUBMITTED TO THE INSURED'S MAJOR MEDICAL CARRIER. Periodontal Maintenance/Periodontal Cleaning PERIODONTAL MAINTENANCE COVERED AS A BASIC SERVICE. THE PLAN COVERS EITHER ONE REGULAR PROPHYLAXIS OR A PERIODONTAL MAINTENANCE IN ANY 6 CONSECUTIVE MONTH PERIOD. Periodontal Maintenance: Date Not Found Periodontics PERIODONTAL SCALING & ROOT PLANING IS LIMITED TO ONE TREATMENT, PER QUADRANT, IN ANY 24 MONTH PERIOD WHEN NEEDED DUE TO GINGIVAL MIGRATION AND BONE LOSS. Periodontal Scaling & Root Planning: Date Not Found Prosthetic Repairs/Rebase & Relines Other Basic Services Major REPAIRS AND MAINTENANCE ARE CONSIDERED MAJOR CATEGORY SERVICES. THIS INCLUDES CODES D2910-D2920, D2980-D2983, D5410-D5422, D5510-D5520, D5610-D5671, D5710-D5761, D5850-D5851, D6092-D6093, D6640, D6930, D6980 AND D9120. LOCALIZED DELIVERY OF ANTIMICROBIAL AGENTS VIA A CONTROLLED RELEASE VEHICLE (E.G. ARESTIN, ACTISITE) IS NOT A COVERED BENEFIT. ORAL CANCER SCREENING (E.G. VIZILITE, VELSCOPE) IS NOT A COVERED BENEFIT. OCCLUSAL/MOUTH/NIGHT GUARDS ARE CONSIDERED ONLY ONCE PER LIFETIME WHEN PERFORMED WITHIN 6 MONTHS OF OSSEOUS SURGERY. 50% No 50% Page 2 of 3 No 03/02/2016 Guardian Anytime Crowns/Inlays/Onlays/Post & Cores/Buildups SINGLE CROWNS ARE CONSIDERED A MAJOR SERVICE SUBJECT TO REVIEW. PLEASE SUBMIT PRE-PROCEDURE RADIOGRAPHIC IMAGES. REPLACEMENT POST & CORES ARE COVERED IF THE EXISTING POST & CORE IS AT LEAST 10 YEARS OLD AND CANNOT BE REPAIRED. REPLACEMENT CROWNS, INLAYS AND ONLAYS ARE COVERED IF THE EXISTING APPLIANCE IS AT LEAST 10 YEARS OLD AND CANNOT BE REPAIRED. Fixed Bridges & Removable Full & Partial Dentures REPLACEMENT PARTIALS, DENTURES AND BRIDGES ARE COVERED IF THE EXISTING APPLIANCE IS AT LEAST 10 YEARS OLD AND CANNOT BE REPAIRED. Implants SURGICAL PLACEMENT OF IMPLANTS IS NOT COVERED. THE PROSTHETIC APPLIANCE PLACED OVER THE IMPLANT WILL BE CONSIDERED IF THE TOOTH WAS EXTRACTED WHILE INSURED WITH THIS GUARDIAN PLAN AND SUBJECT TO ALL OTHER PLAN PROVISIONS. Other Major Services TEETH MUST BE EXTRACTED WHILE INSURED WITH THIS GUARDIAN PLAN TO BE CONSIDERED FOR PROSTHETIC COVERAGE. TMJ Cosmetic Cosmetic Deductible Cosmetic Max Individual Deductible Family Deductible Individual Dental max $50 $50 $150 $150 $1,500 $1,500 Multi-visit procedures are paid on the preparation date. Accumulator and Deductible Summary Accumulator and Deductible Summary In-Network Out-of-Network Maximum Met to Date for Benefit Period $0.00 $0.00 Orthodontic Benefit Met to date $0.00 $0.00 Deductible Met to Date for Benefit Period $0.00 $0.00 MaxRollover Summary Threshold 0 Maximum Rollover Amount 0 Rollover Amount if all Benefits Paid In-Network 0 Maximum Rollover Account Maximum 0 Personal Maximum Rollover Account 0.0 This is a sample of the maximum rollover benefits under this plan. It is not an all inclusive list nor is it a guarantee of the amount of benefits payable. All benefits are subject to the patient's eligibility as defined by the plan on the date services are rendered. Orthodontic Orthodontic Coverage 50% Orthodontic Deductible Waived Individual Lifetime Ortho Max $2,000 19 Orthodontics Age Limit Page 3 of 3 03/02/2016