Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Trichinosis wikipedia , lookup
Onchocerciasis wikipedia , lookup
Sarcocystis wikipedia , lookup
Human papillomavirus infection wikipedia , lookup
Leptospirosis wikipedia , lookup
2015–16 Zika virus epidemic wikipedia , lookup
Oesophagostomum wikipedia , lookup
Schistosomiasis wikipedia , lookup
Influenza A virus wikipedia , lookup
Orthohantavirus wikipedia , lookup
Ebola virus disease wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Hepatitis C wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Neonatal infection wikipedia , lookup
Antiviral drug wikipedia , lookup
West Nile fever wikipedia , lookup
Marburg virus disease wikipedia , lookup
Hepatitis B wikipedia , lookup
Herpes simplex research wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Henipavirus wikipedia , lookup
Herpes simplex wikipedia , lookup
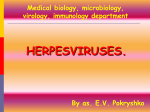
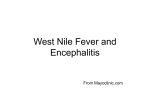
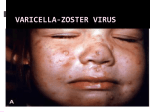
HERPES VIRUS HERPES VIRUS are capable of causing overt disease or remaining silent for many years only to be reactivated, eg shingles. The name herpes comes from the Latin -herpes which, in turn, comes from the Greek word herpein which means to creep. This reflects the creeping or spreading nature of the skin lesions caused by many herpes virus types. There are 25 families in the Herpetoviridae but only eight of them are known to infect man IMPORTANT HUMAN PATHOGENS Herpes simplex virus Type 1 (HSV1) Herpes simplex virus Type 2 (HSV2) Varicella Zoster Virus (VZV) Epstein Barr virus (EBV) Cytomegalovirus (CMV) Herpes lymphotropic virus (HHV6) Human herpes virus 7(HHV7) Human herpes virus 8 HHV8)((Kaposi's sarcoma-associate herpes virus) PROPERTIES OF HERPES VIRUS All are structurally similar • They are DNA, enveloped virus • They are larger 120-200nm in diameter second only to poxvirus • They are the only virus that obtain their envelopes by budding from the nuclear membrane • The virion does not contain polymerase They are noted for their ability to cause latent infections. • STRUCTURE CLASSIFICATION OF HERPES VIRUSES 6 HERPES SIMPLEX VIRUS HSV-1 and HSV-2 Lesion caused by HSV-1 are above the waist while those caused HSV2 are below the waist but both types of HSV can infect oral or genital mucosa depending on the regions of contact. EPIDEMIOLOGY HSV 1 and 2 infections are life long The virus is found in the lesions on the skin and in body fluid HSV-1 is transmitted primarily in saliva can spread by kissing or the use of utensils contaminated with saliva or by transfer of infectious virus to the hands after which the virus may enter the body via any wound or through eyes Anyone who comes in contact with the fluid containing virus is at risk Care workers are affected by disease called herpetic whitlow that results in lesions on the fingers HSV-2 infection is most prevalent in life as number of sexual contact increases Thus the lowest rates of infection are in children PATHOGENESIS The virus replicate in the skin or mucous membrane at the initial site of the infection Then migrate up the neuron and become latent in the sensory ganglion cells HSV 1 becomes latent in the trigeminal ganglia HSV-2 becomes latent in the lumber and sacral ganglia The viruses can be reactivated from the latent by the variety of induces sunlight, hormonal changes, trauma, stress and fever at which time it migrates down the neuron and replicate in the skin causing lesions Diseases caused by HSV-1 and HSV-2 CLINICAL PRESENTATION OF HSV-1 1.Gingivostomatitis occurs in children, • characterized by fever, irritability and vesicular lesions in the mouth • The lesions heal spontaneously in 2-3 weeks • Many children have asymptomatic primary infections • Herpetic gingivitis 2.HERPES LABIALIS (FEVER BLISTERS OR COLD SORES) characterised by crops of vesicles at the mucocutanous junction of the lips or nose Recurrences frequently reappear at the same site • 3.Keratoconjuctivitis Patients with HSV keratitis may complain of • Pain • Photophobia • Blurred vision • Tearing • Redness The earliest sign of active viral replication in the corneal epithelium is the development of small, raised, clear vesicles • recurrence can lead to scarring and blindness 4.Encephalitis • • • Involve the temporal lobe has high mortality rate causes severe neurological sequel in those who survive 5.HERPES WHITLOW • • Is a pustule lesion of the skin of the finger or hand it is most commonly contracted by dental workers and medical workers exposed to herpes lesions Symptoms of herpetic whitlow • include swelling, • reddening and • tenderness of the skin of infected finger. • This may be accompanied by fever and swollen lymph nodes Disseminated infections such as esophagitis and pneumonia, occur in immunocompromised patients with depressed T cell function HSV-2 PRESENTATION 1. Genital herpes • painful vesicular lesions of the male and female genitals and anal area • The lesions are more severe in primary disease than in recurrences • Primary infection is associated with fever and inguinal adenopathy. • Asymptomatic infections occur in both men (in prostate or urethra) and women (in the cervix) it can be the source of infection to other individuals. GENITAL HERPES ON THE PENIS © Australian Herpes Management Forum GENITAL INFECTION IN MALE AND FEMALE 20 HSV PROCTITIS This is an inflammation of the rectum and the anus 2. Neonatal herpes • Originates from contact with vesicular lesions within the birth canal • can be prevented by performing caesarean section on women with either active lesions or positive viral cultures Both HSV1 and HSV2 can cause severe neonatal infections that are acquired after birth from carriers handling the child Despite their association with neonatal infections neither HSV1 nor HSV2 cause congenital abnormalities to any significant degree Aseptic meningitis Caused by HSV2 is usually mild and self limited disease LABORATORY DIAGNOSIS • Isolation of the virus from the lesion by cell culture then detecting virus specific glycoprotein by enzyme-linked immunosorbent assay (ELISA) Diagnosis from skin lesions can be made by the Tzanck smear in which cells from the base of the vesicle are stained with Giemsa stain. • The present of multinucleated giant cells suggests Herpes infection • • Encephalitis can be diagnosed by detecting HSV-1 DNA in the spinal fluid using PCR Neonatal herpes can be diagnosed by use of viral culture or PCR TREATMENT Acyclovir the treatment of choice of encephalitis and systemic diseases caused by HSV-1 also in primary and recurrent genital herpes also neonatal infection caused by HSV-2 It shortens the duration of the lesions and reduces the extent of shedding of the virus Mutant resistant acyclovir have been isolated from patients famciclovir and valacyclovir can be used in this cases PREVENTION Avoid contact with the vesicular lesion or ulcer Caesarean section is recommended for women at term who have positive viral culture VARICELLA ZOSTER VIRUS CHICKENPOX AND SHINGLES This virus causes two major diseases, chicken-pox (Varicella), usually in childhood, and shingles, later in life. Shingles (Herpes zoster) is a reactivation of an earlier varicella infection. CHICKEN POX This virus is highly infectious It is spread by respiratory aerosols or direct contact with skin lesions. PATHOGENESIS The virus infect the mucosa of URT The virus spread from the URT to lymphocytes and monocytes and to the reticuloendothelial system where second viremia occurs and the virus travels to the skin, mouth, conjunctiva, respiratory tract and to epithelial sites throughout the body forming papule containing multinucleated cells with intracellular inclusions. CLINICAL FEATURES Incubation period 14-21 days Brief symptoms of fever and malaise occur Papule vesicular rash then appear in crops on the trunk and spread to the head and extremities. The rush evolves from papules to vesicles, pustules and finally crust. Itching is marked Complications Varicella pneumonia and encephalitis are the major rare complications Reye’s syndrome characterised by encephalitis and liver degeneration esp. in children given aspirin Its pathogenesis is not known ZOSTER (SHINGLES) • • The occurrence of painful vesicles along the course of a sensory nerve of the head or trunk Reactivation can lead to chronic burning or itching pain called post-herpetic neuralgia which is seen primarily in the elderly In immunocompromised patients life threatening disseminated infections such as pneumonia can occur Diagnosis • Most diagnosis are made clinically Treatment • • • No antiviral therapy is necessary for chicken pox or shingles in normal patients Immunocompromised patients can be treated with acyclovir PREVENTION • • • Varicella- zoster immune globulin (VZIG) (effective in preventing varicella but not zoster) There is a live attenuated vaccine (Varivax) for varicella but is not effective in zoster and can not be used for immunocompromised patients or pregnant women chickenpox of the new-born. The infant contracted chickenpox at birth from her infected mother. CHICKEN POX chickenpox rash. Some of the sores are red spots and some are blisters Severe atypical episode of shingles affecting the trunk of a person with impaired immunity Shingles affecting the left side of the trunk Recurrent varicella zoster on the right side of the face Facial shingles. PRESENTATION OF VARICELLA AND ZOSTER CYTOMEGALOVIRUS CYTOMEGALOVIRUS Cause 1. cytomegalic inclusion disease (esp. congenital abnormalities) in the neonates • 2.pneumonia in immunocompromised individuals TRANSMISSION Early in life CMV can be transmitted • across the placenta • within the birth canal • and in breast milk In young children –Via saliva Later in life-sexually transmitted It is present in secretions - saliva, urine, vaginal and semen The virus can also be spread via blood transfusions and transplants. PATHOGENESIS The virus first infects the upper respiratory tract and then local lymphocytes. Circulating lymphocytes then spread the virus to other lymphocytes and monocytes in spleen and lymph nodes. finally spreads to a variety of epithelial cells including those of salivary glands, kidney tubules, testes and cervix. Infection is usually asymptomatic (sub-clinical) CONGENITAL DISEASE There are two instances in which cytomegalovirus can cause serious disease. 1.During a primary infection of the mother (in utero) the virus can spread via the placenta to the fetus and congenital abnormalities can occur; this virus is the most common viral cause of congenital disease. Abnormalities include microcephaly, brain calcification hepatosplenomegaly hearing loss, seizures and mental retardation can occur • • • If the mother has antibody that will neutralize the virus the foetus will not be infected. If the foetus is infected during first trimester congenital defects may result because this is when the organs began to develop 2.Perinatally Besides infection in utero, infants may be infected perinatal As noted above, one tissue in which cytomegalovirus can set up a latent infection is the cervical epithelium and immunosuppression associated with pregnancy can lead to reactivation. Also breast epithelium can harbor latent virus that may be similarly reactivated leading to infection of the infant. Neonates may also receive the virus through infected blood transfusions. In this case, the amount of virus is much higher and symptoms may occur. These usually consist of pneumonia and hepatitis. CLINICAL FINDINGS Approx.20% of infants infective with CMV during gestation show clinically apparent manifestations of cytomegalic inclusion disease such as microcephaly, deafness and jaundice Hepatosplenomegaly is very common Cytomegalic inclusion is the leading cause of mental retardation Infected infant can continue to excrete CMV especially in the urine for several years In immunosupressed adult CMV can cause heterophil-negative mononucleosis which is characterized by fever lethargy and the presence of abnormal lymphocytes in peripheral blood smears Systemic CMV infection especially pneumonitis and hepatitis is high in immunosuppressed patients eg those with renal and borne marrow transplants in AIDS patients CMV commonly affects the intestinal tract and cause intractable diarrhoea. CMV also cause retinitis in AIDS patients which can lead to blindness LAB DIAGNOSIS Cell culture Fluorescent antibody and histologic staining of inclusion bodies in giant cell in urine and in tissue Treatment Ganciclovir is effective in treatment of AIDS patients with pneumonia and retinitis Forscarnet( foscavir) is also effective but cause side effects CMV is resistant to Acyclovir PREVENTION No vaccine Infants who are shedding viruses in their urine should be kept isolated from other infants Blood transmission to new born should be CMV antibody negative if possible only organ from CMV antibody negative donors should be transplanted EPSTEIN BARR VIRUS EPSTEIN BARR VIRUS Epstein-Barr virus is the causative agent of Burkett's lymphoma Nasal pharyngeal carcinoma Oral hairy leukoplakiain lesions in the mouth and Infectious mononucleosis TRANSMISSION AND EPIDEMIOLOGY is transmitted primarily by exchange of saliva e.g. during kissing Is most common infection worldwide Infection in the first few years of life is asymptomatic Is highest in those who are exposed to virus later in life e.g college students PATHOGENESIS The infection first occur in oropharynx and then spread to the blood where it affects B lymphocytes Cytotoxic T lymphocytes react against the infected B cells. EBV remain latent within B lymphocytes CLINICAL FINDINGS Characterized by fever , sore throat, lymphadenopathy and splenomegaly Anorexia and lethargy are prominent Hepatitis is frequent Encephalitis occurs in some patients Spontaneous recovery usually occur in 2-3 wks. In immunosupressed patient infection is severe and is often fatal LAB DIAGNOSIS Hematological approach where abnormal lymphocytes are seen on the smear The EBV-specific antibody test TREATMENT No antiviral therapy is necessary for uncomplicated infections mononucleosis Acyclovir has little activity against EBV but higher doses may be useful in life threatening EBV infections No EBV vaccine OTHER HERPES VIRUSES Human herpes virus 6 This virus is found worldwide is found in the saliva of the majority of adults (>90%). It infects almost all children by the age of two and the infection is life-long. Again, it replicates in B and T lymphocytes, in the oropharynx. Human herpes virus-6 has two forms, HHV-6A and HHV-6B. The latter causes exanthem subitum. symptoms include fever and sometimes upper respiratory tract infection and lymphadenopathy. The symptoms last a few days after an incubation period of around 14 days. EXANTHEM SUBITUM MACROPAPULAR RASH The fever subsides leaving a macropapular rash on the trunk and neck that last a few days longer. This virus may co-infect HIV-infected T4 lymphocytes exacerbating the replication of HIV. Patients with HIV have a higher infection rate than the normal population. HHV-6 has been associated with a number of neurological disorders, including encephalitis and seizures. It has been postulated to play a role in multiple sclerosis and chronic fatigue immunodeficiency syndrome. HUMAN HERPES VIRUS 7 This virus binds to the CD4 and replicates in T (CD4+) cells and is found in the saliva of the majority of the adult population (>75%). Most people acquire the infection as children and it remains with them for the rest of their lives. It is similar to HHV-6 and may be responsible for some cases of exanthem subitum HUMAN HERPES VIRUS 8 This is known as Kaposi's sarcoma associated herpes virus and is found in the saliva of many AIDS patients. It infects peripheral blood lymphocytes. TRANSMISSION Sexually transmitted through semen. Transmitted through mother to child Organ transplant HERPES B This is a simian virus found in old world monkeys but it can be a human pathogen in people who handle monkeys (monkey bites are the route of transmission). In humans, the disease is much more problematic than it is in its natural host. about 75% of human cases result in death with serious neurological problems (encephalitis) in many survivors. There is also evidence that the disease can be passed from a monkey-infected human to another human. In vitro the virus is sensitive to both Acyclovir and Ganciclovir and these are recommended for therapy. Their efficacy is unknown. PAPILLOMAVIRUS PAPILLOMAVIRUS (HPV) - PROPERTIES Non enveloped, DNA virus small 60nm diameter These viruses are very difficult to study as they do not grow in cell cultures and experimental animals. About 70 different types of papilloma virus can infect humans They account for more than 80% of cervical cancers Cause papillomas (benign tumors of squamous cells) e.g. warts on the skin Penile, vulvar and rectal cancers are also associated with HPV. Highly adopted to human skin and mucosa At least 25 types including HPV 6,11,16 and 18 can infect the genital area and are sexually transmitted. HPV 1 and 4 causes plantar warts HPV 2,3 and 10 causes warts on the knees and fingers. Subtypes 6 and 11 account for 90% of genital warts WARTS Warts - - can be Filiform with finger-like projection Flat topped, Flat as they grow inwards due to external pressure (planter warts) A cauliflower-like protuberance (e.g. genital warts) A flat area of dysplasia on the cervix Epidermal dysplasia verruciformis TRANSMISSION By skin to skin contact Genital warts are among the most common sexually transmitted diseases Skin warts are more common in children and young adults and tend to regress in older adults Warts viruses can survive on inanimate objects such as; wrestling mats, towels and shower floors PATHOGENESIS PV infect squamous epithelial cells induce within those cells a characteristic cytoplasmic vacuoles. These vacuolated cells called koilocytes are the hallmark of infection by these virus. The cells grow abnormally and produce warts. Most warts are benign( and do not progress to malignancy PENILE WARTS VAGINA WARTS TREATMENT - WARTS • • Like other tumors, warts can be treated by killing or removing all abnormal cells. To accomplish this; - Wart cells can be destructed by application of karyolitic agents (i.e. salicylic acid) - Freezing with dry ice (solid CO2) or liquid nitrogen. - By burning the tissue with an electrically heated needle - Or by surgical removal Most HPV infections resolve spontaneously For those infected with the high risk subtypes, roughly 5-10% will develop persistent HPV infection It is estimated that 40% of young women are infected with HPV within 3 years of starting sexual activity. Up to 80% of women acquire the HPV infection at least once during their lives. PERSISTENT HPV INFECTION Persistent HPV infection disrupts the normal cell turnover at the transformation zone With the cells multiplying perpetually, pre-cancerous cells form. The pre-cancerous cells could, in the long run, invade underlying tissue: Invasive cancer The process from HPV infection to cancer is very slow taking many years, even decades. SIGNS AND SYMPTOMS • The most common finding in patients with cervical cancer is an abnormal Papanicolaou (Pap) test result. 86 • Physical symptoms of cervical cancer may include Abnormal vaginal bleeding Vaginal discomfort Malodorous discharge Dysuria Because many women are screened routinely, the most common finding is an abnormal Papanicolaou (Pap) test result. Typically, these patients are asymptomatic. • Clinically, the first symptom of cervical cancer is abnormal vaginal bleeding, usually postcoital. vaginal discomfort, malodorous discharge, 87 and dysuria • The tumor grows by extending • along the epithelial surfaces, • both squamous and glandular, • upward to the endometrial cavity, • throughout the vaginal epithelium, • and laterally to the pelvic wall. • 88 • • • • • • • • It can invade the bladder and rectum directly, leading to constipation, hematuria, fistula, and ureteral obstruction, with or without hydroureter or hydronephrosis. The triad of leg edema, pain, and hydronephrosis suggests pelvic wall involvement. The common sites for distant metastasis include extra pelvic lymph nodes, liver, lung, and bone. RISK FACTORS Early age of becoming sexually active Multiple sex partners Unprotected sexual intercourse: condoms estimated to give around 70% protection against HPV. Concomitant STIs PENILE CANCER ANAL CANCER OROPHARYNG EAL CANCER PREVENTION Achieved through regular screening Treatment of pre-cancerous lesions The vast majority of cervical cancer deaths are in developing countries largely because of lack of screening programmes Limited resources (supplies, trained personnel, equipment, quality control, health care infrastructure, and effective follow-up procedures) ? Political will SCREENING: LIQUID BASED CYTOLOGY (LBC) /PAP SMEAR Sample collected using a brush with a detachable head The head with the sample is detached into the specimen pot with the preservative. In the laboratory, the fluid with the sample is spun to separate and remove contaminants e.g. Pus, inflammatory cells and mucus. The remaining cervical cells are then made into a thin layer on a slide and read under a microscope as normal Adoption of this method has reduced the recall rate from 1 in 10 to 1 in 100. Traditional Pap Smear Brush for LBC VISUAL INSPECTION WITH ACETIC ACID (VIA) Also called ‘direct visual inspection’ or cervicoscopy An alternative to cytologic examination in low-resource settings. Involves applying 3-5% Acetic acid (vinegar) to the cervix using a spray or cotton swab. Observe the cervix with a naked eye after 1 minute Obvious acetowhite areas would be regarded as positive for at least pre-cancerous cells. VIA does not require a laboratory or intensive staff training and results are immediately available. Acetowhite Normal cervix VISUAL INSPECTION WITH LUGOL’S IODINE: VILI VILI stands for Lugol’s iodine is applied to the cervix and this is inspected for nonstaining areas. Results of VILI are immediately available, offering the advantage of treatment or follow-up care without delay. OTHER SCREENING METHODS HPV DNA TESTING Detects DNA from 13 high risk genotypes A sample of cells collected from the vagina or cervix using a swab or brush Laboratory processed Very good in identifying those who already have cervical disease and those at high risk of developing it Remains quite expensive ..THE FAST HPV TEST detect DNA from 14 high-risk types of HPV. Results available in 2 - 3 hours The test equipment is portable, with the option of battery power. PRIMARY PREVENTION: VACCINATION Vaccination against the high risk HPV subtypes now available Gardasil® protecting against infection by subtypes 16 and 18 as well as 6 and 11 Cervarix™ protects against subtypes 16 and 18. Both are administered in the form of injections. Three injections given in intervals over a course of six months. HPV VACCINATION Aim is to get girls vaccinated before they become sexually active and exposed to the virus. The vaccines have been shown to be almost 100% effective in preventing dysplasia and subsequent cervical cancer In addition, effective in preventing, the related albeit less common vulvar and vaginal cancers.