Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Microbicides for sexually transmitted diseases wikipedia , lookup
Schistosomiasis wikipedia , lookup
2015–16 Zika virus epidemic wikipedia , lookup
Sarcocystis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Influenza A virus wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Ebola virus disease wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Orthohantavirus wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Hepatitis C wikipedia , lookup
Antiviral drug wikipedia , lookup
Neonatal infection wikipedia , lookup
Oesophagostomum wikipedia , lookup
Marburg virus disease wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
West Nile fever wikipedia , lookup
Hepatitis B wikipedia , lookup
Henipavirus wikipedia , lookup
Lymphocytic choriomeningitis wikipedia , lookup
Herpes simplex research wikipedia , lookup
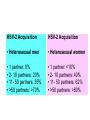
Pornpimol L. INTRODUCTION TO THE FAMILY HERPESVIRIDAE GENERAL CHARACTERISTICS • Herpesviruses are amongst the largest human viruses • HV infections have been recognised since ancient times • “herpein” = “to creep” in ancient Greek (Hippocrates) • Herpesviruses are highly disseminated in nature •. To date, there are 8 known human Herpesviruses. ARCHITECTURE THE HUMAN HERPESVIRUSES Human herpesvirus type 1 (Herpes simplex virus -1) Human herpesvirus type 2 (Herpes simplex virus -2) Human herpesvirus type 3 (Varricella zoster virus) Human herpesvirus type 4 (Epstein-Barr virus) Human herpesvirus type 5 (Cytomegalovirus) Human herpesvirus type 6 Human herpesvirus type 7 Human herpesvirus type 8 Herpes B virus (chimpanzees) may infect humans To date, there are 8 known human Herpesviruses. Alphaherpesvirinae: - variable host range, short reproductive cycle, rapid spread in cell culture Simplexvirus human herpesvirus 1, 2 (HSV-1, HSV-2) Varicellovirus human herpesvirus 3 (VZV) Betaherpesvirinae: - restricted host range, long reproductive cycle, enlargement of infected cells Cytomegalovirus human herpesvirus 5 (HCMV) Roseolovirus human herpesvirus 6, 7 (HHV-6, HHV-7) Gammaherpesvirinae: -replicate in lymphoblastoid cells, specific for T or B cells Lymphocryptovirus human herpesvirus 4 (EBV) Rhadinovirus human herpesvirus 8 (HHV-8) Alphaherpesvirinae Simplexvirus (HHV1&2/ HSV1&2) Varicellovirus (HHV3/VZV) HERPES SIMPLEX VIRUS • First human herpesvirus discovered (1922) • Two serotypes recognised – HSV-1 & HSV2 (1962) • Great deal of polymorphism at genomic level occurs between strains Herpes Simplex Viruses • Herpes Simplex – Two major strains • Type I: Oral Herpes • Type II: Genital Herpes – Skin lesions form at site of the infection – Virus travels along sensory neurons to ganglia , where it remains – During times of stress or weakened immunity , virus may travel along same neurons to re - infect the initial skin sites PATHOGENESIS • HSV-1 infection is generally limited to the oropharynx. Transmission through respiratory droplets • HSV-2 infection is usually acquired by sexual transmission • Virus must come in contact with mucosal membranes or abraded skin for initiation of infection • After primary infection virus is transported to dorsal root ganglia and remains latent • Incubation period of 2-12 days, and symptoms last for 2-3 weeks Clinical Manifestations • HSV is involved in a variety of clinical manifestations which includes ;1. Acute gingivostomatitis 2. Herpes Labialis (cold sore) 3. Ocular Herpes 4. Herpes Genitalis 5. Other forms of cutaneous herpes 6. Meningitis 7. Encephalitis 8. Neonatal herpes HERPES SIMPLEX - Type 1 PRIMARY INFECTION 1. Usually cold sores; sore throat, fever and, rarely, Encephalitis 2. Less frequently found as a genital infection HERPES SIMPLEX - Type 1 TRIGEMINAL NERVE LATENT INFECTION 1. Asymptomatic - No virus or virion proteins produced 2. Viral DNA resides in sensory cells of Trigeminal nerve ganglion HERPES SIMPLEX – Type1 TRIGEMINAL NERVE RECURRENT INFECTION 1. Virus replicates and travels down sensory nerve fiber to infect epithelial cells around the nose and mouth 2. Symptoms are usually a milder form of primary infection HERPES SIMPLEX - Type 2 1. Usually vesicular eruptions on the genitalia 2. Spread by sexual contact 3. Affects both sexes 4. Once associated with cervical carcinoma 5. Less frequently found as Herpes Labialis (cold sores) HSV-2 Acquisition HSV-2 Acquisition • Heterosexual men • Heterosexual women • 1 partner: 0% • 2- 10 partners: 20% • 11- 50 partners: 35% • >50 partners: >70% • 1 partner: <10% • 2- 10 partners: 40% • 11- 50 partners: 62% • >50 partners: >80% Herpes whitlow Herpes keratitis Most common complications are extragenital lesions (20%) and aseptic meningitis (10%) Recurrent HSV-2 infection is generally milder,and complications are rare. Herpes Encephalitis • Age :5-30yrs,>50yrs • 93-96% HSV-1 • Mech : -nasal mucosa/oropharynx cribiform plateorbital,temporal -blood stream -recurrent: reactive of HV trigeminal gg CN v anterior, middle fossa Clinical : fever,headache,ataxia,dysarthria,seizure Herpes Encephalitis • Investigation : – CSF :wbc50-2000 (L),rbc (hemorrhagic necrosis), sugar ,protein – Tissue biopsy – DNA-PCR(sense98%,sp94%) – EEG:unilateral or bilateral periodic focal spike – CT brain :low density contrasted temporal Disseminated HSV • Organ transplantation,CA s/p CMT,AIDS ,severe burn • Liver,kidney,adrenal,spleen,brain ,GI, bone marrow • Clinical :fever, hemorrhagic vessicle,esophagitis ,pneumonitis, renal failure,hepatitis,DIC • Ix: – CBC:wbc ,plt , – Azothemia,low BS – Abnormal EEG,EKG DIAGNOSIS • Both clinical and lab criteria are useful for establishing for diagnosis of HSV infections. • Clinical :multiple vesicular lesions on an erythematous base or herpetic ulceration • Lab : Wright’s,Giemsa’s ,or Papanicolaou’s stain (giant cell or intranuclear inclusions),isolation of the virus in tissue culture or by demonstration of HSV antigen or DNA TREATMENT * Acyclovir Dz. dose Duration (day) Oral ,genital 200mg x 5times/day 400mg x 3times/day 10-14 10-14 Anus 400mg x 5times/day 10-14 Herpetic whitlow 400 mg x 3times/day 7 Meningitis 5mg/kg v q 8 hrs 10-14 Encephalitis 10mg/kg v q 8 hrs 10-14 Disseminated 15mg/kg /day 10-14 TREATMENT(cont.) * Valacyclovir Dz. Oral,genital Recurrent genital keratitis dose 500-1000mg x 2times/day Duration(days) 10-14 500mg x 2times/day 3-5 1%Trifuridine ED q 2 hrs 21 TREATMENT (cont.) • Suppression of Mucocutaneous Herpes • Reduction in Transmission of HSV to sexual partners • Acyclovir resistance ;foscarnet VARICELLA ZOSTER VIRUS Clinical disease recognised in two forms Primary infection - Varicella (Chicken Pox) Reactivation - Zoster PRIMARY VARICELLA PATHOLOGY Clinical disease is usually benign. Manifests as a viral exanthem (rash) Virus enters via mucosa of URT and oropharynx or via the conjunctiva Viral replication occurs in primary site and virus disseminates via the blood stream. Virus replication then occurs in cells of the reticuloendothelial system (blood mononuclear cells) Virus replication is initially limited by specific and nonspecific immunological responses but in most individuals these are overwhelmed and extensive secondary viremia occurs Secondary viremia is associated with prodromal symptoms (fever) which first appear 14-15 days after initial infection Secondary viremia is usually terminated after 3 days by humoral and cell-mediated factors Fever is followed by a maculopapular rash forming lesions over 2-4 days. These may appear on scalp, trunk, extremities and mucosal surfaces. Vesicles contain fluid with infectious virus, and dry over 1-3 weeks. Chicken Pox SECONDARY ZOSTER PATHOLOGY Virus spreads to the ganglia by systemic virus Sets up latent infection in ganglion without replication or cell damage. Reactivation as herpes zoster involves the ganglia and spinal nerves corresponding to the dermatome involved in the primary infection The areas supplied by the trigeminal nerve (opthalmic) and thoracic ganglia are most often involved • Ramsay Hunt :geniculate gg. จะมีอาการปวด และตุ่มน้ าใสบริ เวณหูส่วนนอกมอัมพาตใบหน้าซีกเดียวกันและ สู ญเสี ยความรู ้สึกในการลิ้มรสของลิ้นส่ วนหน้า Lab findings • Isolation of VZV in susceptible tissue culture cell line • Tzank smear • Detection of antibodies:IFA,ELISA,FAMA VZV Encephalitis • 1:1,000 • Children>adult • Clinical:headahe,vomitting,siffneck,siezure ,oculomotor,facial palsy • Dx: – CSF:wbc ,(L) ,prot ,sugar ,Ab positive • Cpx:transverse myelitis,peripheral neuritis,optic neuritis Herpes Zoster ophthalmicus • Occur after zoster eruption in any branch of trigeminal n.(V1) • Produce corneal dendrite • Common sequelae: stromal kerratitis,anterior uveitis,ocular motor n.palsy,acute retinal nerosis,post herpetic neuralgia Treatment Normal host • Chicken pox – prevention of avoidable cpx. ,acyclovir therapy is recommend for adolescents and adult with chicken pox <24hrs(acyclovir 20mg/kg 4times/day x 5) • Herpes zoster – Acyclovir 800mg five times daily for7-10 days Immunocompromised host • Should be treat with intravenous acyclovir(1012.5mg/kg v q8hrs 7days Treatment • Acute neuritis and/or postherpetic neuralgia :gabapentin,amitryptyline,lidocainpatches and fluphenazine hydrochloride • Prevention :Varicella vaccine (active immunization) ,VZIg (passive immunization) Betaherpesvirinae • Cytomegalovirus (HHV5/CMV) • Roseolovirus (HHV6 & 7) HUMAN HERPESVIRUS - 6 First isolated from PBMC of patients in 1986 during attempts to isolate HIV Later isolated from patients in Africa and the UK and subsequently was found to be ubiquitous. Genetic similarity and growth cycle to CMV led to classification as a beta-herpesvirus Two variants of HHV-6 have been identified on basis of genetic and biological properties (variants A and B) Primary Infection • HHV-6 causes exanthem subitum (Roseola) in children - Benign disease - Fever, rash - Complications include febrile convulsions - 60-70% of infections are unapparent - Variant B is predominant cause • Immunocompromised :organ transplantation – Solid organ,bone marrow transplant – Fever,headache,confusion,seizure,abnormal movement and behavior change – CSF ;PCR DIAGNOSIS • Children(primary infection) :antiHHV-6,fourfold rise of antiHHV-6 IgG • Clinical & HHV-6 in PBMC and plasma,high viral load TREATMENT • ในเด็กที่ภูมิคุม้ กันปกติมกั หายได้เอง • immunocompromisid : ganciclovir,foscarnet,cidofovir Gamma herpesvirinae • Epstein Barr Virus • Kaposi’s sarcoma associated herpesvirus (KSHV) KSHV • Human herpes virus 8(HHV-8) or Kaposi’s sarcoma associated herpes virus (KSHV) • Associate with multicentric Castleman’s dz. and primary effusion lymphoma • “Rhadinovirus” • Risk in AIDS>normal population 20,000x • Homosexual PATHOGENESIS • Oral transmission (saliva), fecal-oral sexual contact and parenteral transmission Clinical manifestation • • • • Classic KS : “Kaposi’s sarcoma” Endemic or African KS Iatrogenic KS AIDS-associated KS AIDS-Associated KS • AIDS defining illness • Skin lesion;รู ปร่ างรี เรี ยงตัวตามskin tension line symmetrical ตามหน้า,ขาและอวัยวะเพศ (maculepappules/nodules) • Pulmonary KS • Gastrointestinal KS Kaposi’s sarcoma Staging of AIDS associated KS Disease associate with HHV-8 • • • • • Pemphigus Interstitial pneumonitis Hemophagocytic syndrome Multiple myeloma Kikuchi’s dz.( Histtocytic necrotizing lymphadenitis) DIAGNOSIS • Molecular – PCR – In situ hybridization – immunohistochemistry • Serology – IFA – ELISA TREATMENT • Palliation – Localized dz :radiation, vinblastin,interferon, tumor necrotic factor – Systemic therapy: extensive mucocutaneous dz. , visceral organ dz., lympedema,painful local lesion >>bleomycin ,doxorubicin ,daunorubicin, etoposide,paclitaxel * (cidofovir,foscarnet and gancyclovir)