Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
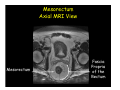
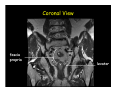
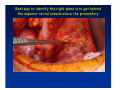
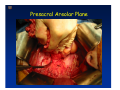
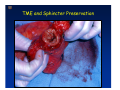
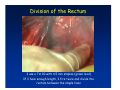
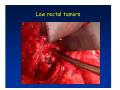
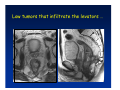
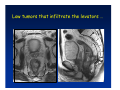
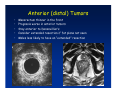
Kaiser Permanente 4th Annual National Surgical Symposium April 2008 Ojai, California Technical Pearls for Rectal and Pelvic Surgery Julio Garcia-Aguilar Professor of Surgery Chief, Section of Colon and Rectal Surgery Department of Surgery University of California, San Francisco Important Issues • • • • • know the anatomy stage the tumors appropriately develop a "game" plan have proper instrumentation get adequate help Simple instrumentation…. Or not so simple…. Anatomy • rectum and mesorectum • pelvis • pelvic floor muscles Mesorectum • Visceral mesentery surrounding the rectum • Derived from the dorsal mesentery of the hindgut • Covered by the fascia propria of the rectum • Contains: – branches of the superior rectal vessels – perirectal lymph nodes Mesorectum Axial MRI View Mesorectum Fascia Propria of the Rectum Mesorectum • Connected to pelvic sidewall by the lateral stalks – a condensation of the endopelvic fascia • The lateral stalks may contain accessory middle rectal vessels; the middle rectal artery runs immediately above the levators • The mesorectum tapers distally toward the hiatus of the puborectalis • The very distal portion of the rectum – the anorectal ring – is devoided of mesosrectal fat Mesorectum • Thinner in the front, compared to sides and the back • Separated from urogenital organs by Denonvillier’s fascia – a remnant of the embryological cull de sac • The fascia propria of the rectum not very clearly visualized anteriorly Sagital view Mesorectum Bladder Pubis Prostate Levator Sphincter Coronal View fascia propria levator Some facts… • The holy plane is the “only” plane to perform an anatomical excision of the rectum • Any other plane makes surgery technically more difficult and increases the risk of bleeding, injuring other organs, and tumor recurrence • Total mesorectal excision can be safely done by an open, laparoscopic or robotic approach • Use sharp dissection – electrocautery works well Principles • Best way to identify the right plane is to get behind the superior rectal vessels above the promontory • It is important to pay attention to the hypogastric plexsus that runs in front of the bifurcation of the aorta • Pulling the superior rectal vessels forward stretches the areolar tissue that connects the fascia propria of the rectum to the promontory and opens the entrance to the “holy plane” Best way to identify the right plane is to get behind the superior rectal vessels above the promontory It is important to pay attention to the hypogastric plexus that runs in front of the bifurcation of the aorta Pulling the superior rectal vessels forward stretches the areolar tissue that connects the fascia propria of the rectum the promontory and open the entrance to the “holy plane” Presacral Areolar Plane Start the dissection posteriorly and continue as far as you can Visualize and preserve the hypogastric nerves as they course laterally and distally Work from posterior to anterior opening the peritoneum in both sides of the mesorectum all the way to the cull-de-sac. Divide the lateral stalk keeping in mind the pelvic plexus – they usually contain accessory branches of the middle rectal In cancer patients continue the anterior dissection in front of Denonvillier’s Surgical Specimen TME and Sphincter Preservation Division of the Rectum I use a TA 30 with 4.5 mm staples (green load) If I have enough length, I fire twice and divide the rectum between the staple lines Special Circumstances… • The high tumor • The very distal tumor • The anterior tumor The Cancer of the Upper Rectum Do we need to excise the entire mesorectum in every rectal cancer? Distal Mesorectal Spread in TME Specimens • 50 rectal cancer patients treated by TME • No mesorectal tumor deposits in 6 T2 tumors • Mesorectal/nodal deposits in 28 of 44 (64%) T3 tumors – 12 with mesorectal deposits distal to tumor – 5 with mesorectal deposits more than 2 cm distal to tumor – 1 with mesorectal deposits more than 5 cm distal to tumor Reynolds et al, BJS 1996 Distal Mesorectal Spread Increases with Tumor Penetration • 20% mesorectal tumor deposits distal to tumor – 12% for T3 tumors – 25% for T4 tumors • No tumor deposits beyond 5 cm from tumor Hida et al, JACS 1996 Total vs. Partial Excision of the Mesorectum • Evidence: retrospective analysis • Cancers of the upper rectum treated by partial excision of the mesorectum have the same local recurrence rate than rectosigmoid cancers » Lopez-Kostner et al, Surgery 1998 • No difference in local recurrence between upper rectal tumors treated by partial mesorectal excision and mid and lower rectal tumors treated by total mesorectal excision » Bokey et al, Br J Surg 1999 “Tumor Specific” Mesorectal Excision • Sharp excision • Complete excision of the mesorectum for cancers of the mid and distal rectum • Transection of the mesorectum 5 cm below the lower margin of the tumor for cancers of the upper rectum • No conning to the distal resection margin Low rectal tumors For “very” low tumors… • Anterior tumors that do not infiltrate the prostate or vagina, levators or anal sphincter • Have responded to neoadjuvant chemoradiation • You are uncertain about being able to place the TA stapler and ensure adequate margin • Do a transanal – transabdominal resection with direct vision of the distal margin Transanal – Transabdominal Approach • Star with the patient prone • Make a full-thickness circumferential incision in the bowel wall at or slightly above the dentate line – you should see the lower margin of the tumor (leave 1 cm margin) • Dissect the rectal wall from the surrounding tissues – prostate anteriorly, puborectalis laterally, and levator posteriorly • Carrie the dissection several centimeter proximally • Close the lumen of the rectum with interrupted sutures Transanal dissection Transanal – Transabdominal Approach (cont) • Transfer the patient to the lithotomy position • Do your total mesorectal excision until you reach the dissected area down in the pelvis • If you do it laparoscopically you could remove the specimen through the anus, and avoid an abdominal incision • Do your hand-sewn colo-anal anastomosis • Loop ileostomy Transanal removal of specimen Transanal Intersphincteric If the tumor infiltrates the levator or the sphincter before neoadjuvant therapy, the patient should probably have an APR Low tumors that infiltrate the levators … Low tumors that infiltrate the levators … Abdominoperineal Excision APR Specimens - No conning!! From Marr et al, Ann Surg 242, 2005 Anterior (distal) Tumors • • • • • Mesorectum thinner in the front Prognosis worse in anterior tumors Stay anterior to Denonvillier’s Consider extended resection if fat plane not seen Males less likely to have an “extended” resection Up to 12% of rectal cancers extend beyond the structures that are normally removed with a total mesorectal excision Postoperative chemoradiation does not prevent recurrence if the circumferential resection margin is involved by tumor Organs Involved • • • • • • Urinary System Male genital system Female genital system Small bowel Sacrum Pelvic side walls Fixation to Adjacent Organs • Direct tumor infiltration in ~ 50% of cases • Due to inflammatory adhesions in ~ 50% of cases • Impossible to distinguish tumor infiltration from inflammatory adhesions Facts • Separating tumor from adjacent organs associated with high tumor recurrence rates • En block resection associated with less recurrence and better survival, in spite of higher operative morbidity Avoid facing a multivisceral resection when the surgeon and the patient are unprepared Diagnosis • Suspect from H & P – Urogenital symptoms predictors of involvement in 93% of cases – Digital exam not very accurate in identifying colorectal cancer invasion to adjacent organs • Confirm diagnosis by endoscopy • Determine extension by imaging studies Efficacy in Assessing Invasion of Adjacent Organs • Ultrasound • CT • MRI 44% to 94% 64% 75% Limitations of Imaging Studies in Advanced Rectal Cancer • Most patients with an advanced rectal cancer receive preoperative chemoradiation • Preoperative images not comparable to pathology • Imaging studies unable to distinguish post-treatment fibrosis from residual tumor Decisions regarding the extent of resection in patients with locally advanced rectal cancer must be based on the pre-treatment images Tumor Infiltrating Bladder CT Scan MRI Patient Selection • Patient related issues – Performance status – Co-morbid conditions • Extension of the disease – Local extension – Metastasis Resection Margins Three Anatomical Planes Anterior: the urogenital organs Lateral: ureters, iliac vessels, side wall Posterior: sacrum, piriformis, sacral plexus Anterior and Posterior Margins Lateral Margins Involved Free The plane beyond the mesorectum Lateral Pelvic Wall Involvement only 17 (31%) of 55 patients with T4 rectal cancer Curative Resection Involved Non-involved Survival 6% 13 months 92% 49 months Yiu et al, DCR 2001 Preoperative Considerations • Plan de operation • Multidisciplinary approach Urology Intraoperative Radiation Plastic surgeon • Prepare OR team Operative Decisions • Exclude intra-abdominal spread • Assess resectability; if you think you cannot remove the tumor, don't try • Start your dissection in planes that you think should be normal based on proeperative imaging • Work around the tumor • Avoid open anatomical planes potentially involved by tumor Operative Decisions • En-block (total or partial ) resection of adjacent organs • Take frozen sections • Identify potential positive margins • Don't think about the reconstruction; leave it to the urologist and plastic surgeon Results of Surgery for Locally Advanced Rectal Cancer • Recurrence 7% to 33% • Survival 31% to 80% • Complications 11% to 79% Multivisceral Resection No Adjuvant Therapy Moriya et al, Colorectal Dis 2003 • 128 patients with T4 rectal cancer • 23% required pelvic exenteration • 1.6% operative mortality • 27% morbidity • 33% recurrence • 57% survival Multivisceral Resection And Neoadjuvant Therapy • • • • • • • Sanfilipo et al, IJRBP 2001 45 patients with T4 tumors by CT or ERUS 5-FU based chemoradiation 13 never had surgery 14 of 32 (41%) had invasion of adjacent organs 20% local recurrence 69% survival Management of the Urinary System • Extensive resections often requires complex reconstruction and permanent urinary diversion • Partial excision my compromise cure without reducing morbidity • Urinary leaks common after chemoradiation Management of the Urinary System • 101 patients with locally advanced or recurrent colorectal cancer • complete cystectomy or prostatectomy better results than partial resection • ureteral invasion was an ominous sign Stief, European Urol 2002 Gender Differences in Treatment? • 282 patients undergoing APR at MSKCC – 15% of females had vaginectomy – 4% of males had prostatectomy • Are we less aggressive in males? • Can this explain gender differences in local recurrence? Complications after Multivisceral Resections • Probably higher than after simple resection • Survival similar if resection RO in both groups • Most common complications: – sepsis – delayed wound healing – fistulas Perineal Wound Complications • Infection/separation in 13% to 79% • Rate increases if: – preoperative radiation – total pelvic exenteration – sacrectomy • Musculocutaneous flaps reduce the rate of complications (79% to 46%, Ko et al surgery 2001) – Rectus muscle – Gluteus – Gracilis Summary • Identify patients before start treatment • Treatment decisions based on initial imaging studies • Multidisciplinary approach • Initial surgery provides the best opportunity for cure • Cure is possible if the tumor can be totally removed Conclusions • A sharp excision following the areolar space outside the fascia propria of the rectum is the optimal surgical technique to perform a radical proctectomy. • This procedure can be now be equally performed by open, laparoscopic, or robotic approach. • A total mesorectal excision should be the standard surgical procedure for cancers of the mid and distal rectum that require a radical operation. • Transection of the mesorectum 5 cm distal to the lower mural margin of the tumor is acceptable for cancers of the upper rectum.