Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
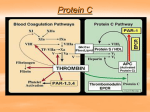
Basics in hemostasis Pocket card Issue number 1 2012 Basics in hemostasis Hemostasis is a complex process which controls bleeding within the finely tuned interplay of procoagulant, anticoagulant, fibrinolytic, and antifibrinolytic activities. It relies on the combined activity of endothelial, platelet, and plasma factors, which are closely regulated to balance the risk of excess bleeding (hemorrhage) against the risk of blood clot formation (thrombosis). Overview of wound repair Stage Mechanism Result 1 Caused by direct injury to the blood vessel, release of vasoconstrictor chemicals by platelets and the endothelium at the site of the injury, and reflex actions indicate kidney damage or disease. Damage to the endothelium exposes subendothelial proteins (e.g. collagen) which attract and tether platelets at the site of the damage (adhesion) Bound and activated platelets release vasoactive and chemotactic agents (e.g. serotonin, adenosine diphosphate or ADP, thromboxane A2) Result of the coagulation cascade is the production and cross-linking of fibrin to form a stable clot (thrombus) at the site of injury A range of factors act to control the action of plasmin, which breaks down fibrin Various Limits the flow of blood to the area of injury to help prevent blood loss Vascular spasm 2 Platelet aggregation: Primary hemostasis 3 Initiation of coagulation cascade 4 Stabilisation of primary clot: Secondary hemostasis 5 Fibrinolysis 6 Wound healing Forms a primary plug made up of loose platelets Attracts more platelets and initiates coagulation cascade Seals the damage until the blood vessel wall can repair or regrow Dissolution of the clot following repair Restores normal viability of the vessel and allows normal blood flow to resume Primary hemostasis (simplified) 4 3 2 1 Endothelial cell Red blood cell Activated platelet Collagen Platelet von Willebrand factor Key factors in hemostasis Factor number or name Synonym Function Coagulation factors I Fibrinogen Precursor of fibrin II Prothrombin III Tissue factor V Proaccelerin Labile factor VII Proconvertin VIII Antihemophilic factor/globulin Christmas factor Precursor of thrombin and main enzyme of coagulation Converts fibrinogen to fibrin Vitamin K dependent Lipoprotein expressed on the membrane of certain cells (e.g. fibroblasts, skin epithelial cells) Binds factor VIIa which initiates the tissue factor/extrinsic pathway Activated to factor Va which acts as a cofactor for the enzyme factor Xa that cleaves prothrombin to thrombin Present in granules in platelets Binds to tissue factor to initiate the tissue factor/extrinsic pathway Vitamin K dependent Activated form (VIIIa) is a cofactor for the intrinsic activation of factor X Activated to factor IXa which is the enzyme responsible for factor X activation Vitamin K dependent Activated to factor Xa, the key enzyme in the final common pathway that activates prothrombin Vitamin K dependent Activated to factor XIa which activates factor IX Calcium dependent Activated to factor XIIa by surface contact, kallikrein or other factors Triggers the prothromin time (PT)-based contact activated/intrinsic pathway Activated by thrombin Cross-links and stabilises the fibrin clot Circulates in a complex with factor XI and acts as a cofactor IX X Stuart-Prower factor XI Plasma thromboplastin antecedent Hageman factor XII XIII High molecular weight kininogen Prekallikrein Fibrin stabilising factor Fitzgerald, Flaujeac or William factor Fletcher factor Participates at the beginning of the contact activated/intrinsic pathway Regulatory/other factors von Willebrand factor vWF Thrombinactivated fibrinolysis inhibitor (TAFI) Carboxypeptidase B2 Tissue factor pathway inhibitor (TFPI) – Protein C – Protein S – Thrombomodulin Antithrombin – – Plasmin D-dimer Associated with subendothelial connective tissue; serves as a bridge between platelet glycoprotein GPIb/IX and collagen Inhibits fibrinolysis by inhibiting binding and activation of plasminogen Activated to factor XIIa by surface contact, kallikrein or other factors Triggers the PTT-based contact activated/ intrinsic pathway Inhibits the cofactor activities of factors VIIIa and Va Vitamin K dependent Cofactor for protein C Vitamin K dependent Endothelial cell binding site for thrombin which, when bound, activates protein C Most important coagulation inhibitor; controls activities of thrombin, and factors IXa, Xa, XIa and XIIa Inactive precursor (plasminogen) is activated by tissue plasminogen activator and functions to digest fibrin Fibrin degradation product Small protein fragment present in the blood after a blood clot is degraded by fibrinolysis The classical coagulation cascade* INTRINSIC Unphysiological surfaces EXTRINSIC Lesion Platelet Contact activation aggregation (collagen, cell fragments, glass) Tissue factor (TF) TFPI Thrombin XII XIIa XI VIIa XIa Ca2+ IX VIII VII Ca2+/PL IXa Prot. Ca/Prot. S IX Ca2+/PL AT III VIIIa X V Ca2+/PL Xa Prot. Ca/Prot. S X Ca2+/PL AT III Va Prothrombin XIII Ca2+ Thrombin XIIIa AT III Fibrinogen Fibrins FibrinI Ca2+ A B TAFIa Fibrinopeptides Plasminogen Fibrin degradation products Plasmin Plasminogen activator Blood coagulation cascade with certain regulatory elements Fibrinogen = factor I Prothrombin = factor II * T his model was developed in vitro and is now known not to reflect in vivo coagulation Cell-based model of coagulation* Initiation Xa TF - VI Ia X Amplification Thrombin IXa TF - VIIa Free vWF Prothrombin Va IX Propagation XI Fibrinogen XIII VIII/vWF Prothrombin V Villa Thrombin XIIIa XIa X Tissue factorexpressing cell Va XIa P-selectin IXa VIlla Xa Va Fibrin activated platelet CD40L PAR 1;4 Gp IIb/IIIa P2Y12/ADP De Caterina et al. Eur Heart J 2007;28:880-913. ©The European Society of Cardiology 2007; with permission of Oxford University Press * T his more recent model is considered to more accurately reflect in vivo coagulation Fibrinolysis Tissue plasminogen activator Factor XIa, XIIa, Kallikrein Plasminogen Plasminogen activator inhibitors α2-antiplasmin Urokinase Thrombin-activated fibrinolysis inhibitor Thrombin Plasmin D-dimer Fibrin Inhibits Other fibrin degradation products (FDPs) Activates Fibrinolysis is a process with the main function to dissolve fibrin clots in blood vessels. The fibrinolytic system allows the body to clear clot fragments safely which avoids the risk of floating clots. Floating clots can cause serious damage to the lungs, the heart and brain. Fibrinolysis comprises a proenzyme, plasminogen, which can be converted to the active enzyme plasmin. Plasmin cleaves the fibrin clot into smaller fragments that can then be expelled by the body and detected i.e. by modern D-dimer tests. Coagulation disorders Disorder Associated abnormality Prevalence* Hemophilia A Factor VIII deficiency Hemophilia B Factor IX deficiency 6.6–12.8 in 100,000 males 1.2–2.7 in 100,000 males 1 in 100,000 Hypocoagulation Inherited Hemophilia C Factor XI deficiency von Willebrand disease von Willebrand factor (vWF) deficiency Defect or deficiency in glycoprotein (GP)Ib, the receptor for vWF Factor V deficiency Bernard-Soulier syndrome Factor V deficiency (parahemophilia/ Owren parahemophilia) Factor X deficiency Congenital dysfibrinogenemia/ afibrinogenemia Factor X deficiency; amyloidosis Abnormality in fibrin (factor I); can result in bleeding disorders or in thrombotic tendency; many subtypes named after the cities in which they were first described (Amsterdam, Detroit, Wiesbaden) Up to 1 in 100 <1 in 1,000,000 1 in 1,000,000 1 in 500,000 1 in 1,000,000 Acquired Disseminated intravascular coagulation (DIC) Vitamin K deficiency Liver failure Acquired dysfibrinogenemia Dysregulation of coagulation and fibrinolysis due to various causes (e.g. bacterial toxins, some cancers) Disturbed gastrointestinal uptake of vitamin K; dietary deficiency Decreased production of coagulation factors by the liver Abnormality in fibrin; most commonly associated with severe liver disease; can result in bleeding disorders or in thrombotic tendency Approx 1 in 100 of all hospitalised patients Variable depending on underlying cause Variable depending on underlying cause Variable depending on underlying cause Hypercoagulation Inherited Factor V Leiden Mutation in factor V that stops inactivation by protein C Congenital thrombophilia Various types, including antithrombin III eficiency, protein C deficiency, protein S deficiency, abnormalities in fibrinogen Up to 5 in 100; clinical outcome varies according to whether patient is homozygous or heterozygous for the mutation Unknown overall Acquired Antiphospholipid syndrome (Hughes syndrome) Antibodies to cell membrane phospholipids Heparin-induced thrombocytopenia (HIT) Immune reaction to heparin 1–5 in 100 have antiphospholipid antibodies; prevalence of syndrome unknown Incidence approx 1–5% in patients treated with heparin * Per given number of the general population unless otherwise stated Summary of standard hemostasis tests The following lists some commonly used global hemostasis tests. Not all tests are included, and not all tests listed will be required for all patients. Reference ranges vary depending on the assay used and therefore may be laboratory specific Prothrombin time (PT) •Measure of the performance of the extrinsic/tissue factor and common pathways •Performed on blood plasma; time to clot after addition of tissue factor (factor III) •Generally reported as international normalised ratio (INR) •INR relates the results obtained with a test and normal sample under particular analytical conditions to standardise between analytical systems: INR = PTtest PTnormal ISI Where ISI = International Sensitivity Index (as given by manufacturer) •Reference ranges: PT ~10–14 seconds (variable depending on assay) INR 0.9–1.2 (2.0–3.0 for patients on warfarin) Partial thromboplastin time/activated partial thromboplastin time (PTT/aPTT) •Measure of the performance of the intrinsic/contact activated and common pathways •Performed on blood plasma; time to clot after addition of phospholipid and an activator •Reference range: 25–93 seconds (variable depending on assay). Shortening of PTT has little clinical relevance Thrombin time •Measure of hemostatically active fibrinogen. Also reflects presence of heparin/heparin-like substances •Performed on blood plasma; time to clot after addition of thrombin •Reference range: <22 seconds (variable depending on assay) Fibrinogen •Measure of clotting ability •Reference range: 200–400 mg/dL (variable depending on assay used) Platelet function test •Measure of platelet function. Used to assess abnormal bleeding (e.g. easy bruising, menorrhagia, epistaxis). Also used to monitor antiplatelet therapy •Various assays available D-dimer •Assesses fibrin deposition and stabilisation (i.e. clot formation) •Used to help diagnose conditions such as venous thromboembolism (VTE) and disseminated intravascular coagulation (DIC). Also used to guide thromboprophylaxis PT result PTT result Condition Prolonged Normal Normal Prolonged Prolonged Prolonged Normal Normal or slightly prolonged Liver disease; vitamin K deficiency; decreased or defective factor VII Decreased or defective factor VIII, IX or XI (hemophilia); von Willebrand disease; lupus anticoagulant (delays in vitro coagulation) Decreased or defective factor I, II, V or X; severe liver disease; disseminated intravascular coagulation May indicate normal hemostasis, but tests may be normal in mild forms of deficiencies