Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
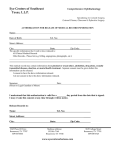
PLACE LABEL HERE CARDIAC STRESS TESTS INFORMED CONSENT (This form is designed to comply with the Georgia Informed Consent Law O.C.G.A. 31-9-6.1) Important: Do not sign this form without reading and understanding its contents. The diagnosis requiring this procedure is: 1. Chest Pain Abnormal ECG or ETT Decreased exercise tolerance Diabetes Difficulty breathing/ Shortness of Breath Dizziness Elevated cardiac enzymes Fainting (syncope) Hypertension Arrhythmias Palpitations Other: _____________________ The nature of the procedure is: Exercise Stress Test –The test will be performed on a treadmill with the amount of effort increasing slowly as the speed and slant increase until symptoms such as fatigue, shortness of breath or chest discomfort occur, or until such time when the provider determines the test to be complete. The patient will notify the provider of any such symptoms. Heart rate and rhythm are constantly monitored on a special heart monitor and periodic blood pressures checked by a cardiology stress technician. OR Pharmacologic Stress Test – If it is unlikely a high enough level of exercise can be reached for the test to be accurate, the provider may suggest a ‘medicated (pharmacologic) stress test’ using Lexiscan (regadenoson), dobutamine or adenosine. These medications will cause the blood flow to the heart to increase as though you were exercising. 2. The purpose of this procedure is to help the doctor in making a diagnosis and deciding on a course of treatment. 3. THIS TEST INVOLVES THE MATERIAL RISK OF ALLERGIC REACTION, ABNORMAL BLOOD PRESSURE, FAINTING, CHANGES IN HEART RHYTHM AND RATE AND IN VERY RARE INSTANCES HEART ATTACK, STROKE AND DEATH. EMERGENCY EQUIPMENT AND TRAINED PERSONNEL ARE PRESENT TO DEAL WITH UNUSUAL SITUATIONS WHICH MAY ARISE. ADDITIONAL RISKS: In addition to the material risks listed above, there may be other potential risks involved in the procedure including, but not limited to the following: Local irritation, bleeding infection and bruising at IV site, and other risks such as: _________________ __________________________________________________________________________________ 4. The likelihood of success of this procedure is: Good *2-17671* FORM 2-17671 REV. 08/2012 Fair Poor Page 1 of 2 PLACE LABEL HER CARDIAC STRESS TESTS INFORMED CONSENT (This form is designed to comply with the Georgia Informed Consent Law O.C.G.A. 31-9-6.1) 5. The practical alternatives to this are: Coronary Angiogram, Stress Echocardiogram and Other: ____________________________________ These alternatives have been discussed. Yes No 6. If I choose not to have the above procedure, by prognosis (future medical condition) may include: Worsening and increase in the seriousness of my condition Heart attack and/or stroke Death Other: __________________________________________________________________________ 7. I understand that the practice of medicine is not an exact science and that NO GUARANTEES OR ASSURANCES HAVE BEEN MADE TO ME concerning the results of this procedure. 8. I have been given ample opportunity to ask questions and any questions I have asked have been answered or explained in a satisfactory manner. By signing this form, I acknowledge that I have read or had this form read, and/or explained to me in general terms, and that I fully understand its content. All blanks or statements requiring completion were filled in and all statements I do not approve of were stricken before I signed the form. I hereby voluntarily request and consent for Dr. __________________________, as my physician, and any other physician(s), and such associates, assistants or other medical personnel involved in performing such procedure(s), to perform the procedure(s) described or referred to herein. __________ Date _________ Time ________________________________ Person giving consent ____________________________ Relationship to patient Patient unable to sign because of _____________________________________________________________ Witnessed by: __________ _________ Date Time at the direction of FORM 2-17671 REV. 08/2012 _______________________________________ Signature of person obtaining consent ________________________ Name of Responsible Physician Page 2 of 2