Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac surgery wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Myocardial infarction wikipedia , lookup
Electrocardiography wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
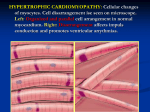
Clinical and electrocardiographic features The first presenter was Dr Kristina Haugaa from Oslo University Hospital in Norway, who talked about clinical and electrocardiographic features and differences between athletes. HCM has a reported prevalence of 1:500 and is a substantial contributor to sudden cardiac death in young athletes. Diagnosis of HCM is made by echocardiography and defined as septal wall thickness > 15 mm in the absence of history of hypertension or other explanatory etiologies, according to Dr. Haugaa. Hypertrophic cardiomyopathy is caused by mutations in genes encoding sarcomeric proteins and has autosomal dominant inheritance. She stressed that genetic testing is recommended in HCM patients and the yield of genetic testing is approximately 50%. A positive test facilitates family screening and follow-up, whereas a negative test does not exclude the diagnosis of HCM. Mild HCM can be challenging to differentiate from athletes’ hearts. Dr Haugaa stressed that an even bigger challenge is to evaluate whether an athlete with left ventricular (LV) hypertrophy may have underlying HCM. To discriminate the two entities, evaluation includes family history, ECG, exercise testing, echocardiography with stress test, cardiac magnetic resonance imaging (MRI) and genetic testing. Examples of features are that septal thickness rarely exceeds 15 mm in athletes and hypertrophy is symmetric. On ECG, HCM patients and athletes both show increased QRS voltage, which is frequently accompanied by bizarre ST-T changes in HCM, but not in athletes. Ethnic differences must also be considered in the evaluation of the ECG, since black athletes have more ECG changes than Caucasians. Different echocardiographic patterns of left ventricular hypertrophy The second presenter was Dr Nico Van de Veire from Ghent in Belgium, who told us that echocardiography has a central role in the detection and quantification of left ventricular hypertrophy (LVH). LVH can be caused by several clinical conditions including arterial hypertension, aortic stenosis, endurance training, hypertrophic cardiomyopathy and some rare conditions. Echocardiography together with clinical information, ECG and other imaging conditions will help the clinician in the diagnostic workup. For this, a comprehensive echocardiographic examination is necessary, focusing on left ventricular and right ventricular function and structure, diastolic function and evaluation of the cardiac valves. Prof Van de Veire highlighted the echocardiographic features of these conditions in his talk. Additional value of contrast-enhanced cardiac magnetic resonance Cardiac MRI is very helpful to distinguish athlete’s heart from CHM according to Prof Berhard Gerber from Woluwe-St. Lambert in Belgium. He stressed that most athletes present with eccentric hypertrophy, characterized by increased LV enddiastolic volume index (EDVi) and right ventricular EDVi, homogenous wall thickening <13mm and maintained LV EDV/mass and wall-thickness/EDV. He convinced us that young athletes never present with late enhancement. However, late enhancement on cardiac MRI is a typical finding in HCM and other pathologies, and predicts worse outcome in these diseases. Therefore, late gadolinium enhancement can be an important factor to help distinguish athlete’s heart from HCM. Overlap of pathologies may exist, however, and there may be questions about the effect of performance-enhancing drugs (doping) on LV remodeling in athletes. Detraining and reversal remodelling The last presenter was Prof. François Carré from Rennes in France. He taught us that detraining will mainly result in a decrease of LV wall thickness and has less effect on LV dilatation. The detraining effect is in favor of athlete’s heart, but even an athlete’s heart might not decrease in thickness during detraining. Detraining must be completed without any significant physical training. Detraining must have a duration of 6 weeks to 6 months before we can review the results and the patients must be studied on a regular basis. He told us that cardiac MRI is probably better than echocardiography to evaluate the results of detraining. Conclusion The session was very informative about this difficult topic and the audience was active and had many questions for the presenters.