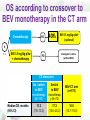
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Recurrent disease Eric Pujade-Lauraine Hôtel-Dieu, Paris, France What is standard? 4rd International Ovarian Cancer Consensus Conference Vancouver, June 25-27, 2010 5th Ovarian Cancer Consensus Conference Tokyo, November 7-9, 2015 Standard in recurrent disease will not take into account • Specific histology • Frail patients: age, comorbidities, … • Patient wish News of the recurrence • Patient opinion: « In some ways, news of the recurrence was almost devastating than the initial diagnosis. My hope of being cured was shattered. I was terrified that the cancer was back, and that it was the beginning of the end »1 1-Ferrel B et al. Cancer 2003 98,5; 1061-71 Advanced Ovarian Cancer: A “chronic” disease with multiple relapses 1°line Platinum-sensitive relpases Platinum resistant relapses Chemotherapy CA-125 Surgery Occlusion 4 months Symptoms PFI: 12 months PFI, platinum-free interval 8 months A collapse of patient beliefs and lifestyle How to prevent recurrence ? • positive attitude (82.5%), • close medical follow-up (82.0%), • vitamins or other supplements (82,0%) • healthy lifestyle (69.0%), • stress reduction (66.5%), • diet (63.0%), • and exercise (58.5%). Stewart DE et al. Medscape 2001 oct Listen to my hopes I am hoping 1. Just for a less painful course of sickness 6% 2. For no recurrence of tumor-related symptoms 35% 3. To live longer than I otherwise would 24% 4. For complete healing without any further complications 28% Oskay-Özcelik G, et al. J Clin Oncol, 2013;31(Suppl): Abstract 5569. Adjusting Hope With Reality • Disparity of expectation and perceived benefit from treatment is correlated with scores of depression Sjoquist KM, et al. Oncologist. 2013;18(11):1221-1228. • Interventions to proactively reduce patient stress, anxiety and/or depression should be considered1 Should it be standard? 1-Lebel et al. J Cancer Surviv 2014 485-96 SURGERY What is the role of cytoreductive surgery for recurrent ovarian cancer? 4th Ovarian Cancer Consensus Conference June 25 – 27, 2010 Vancouver, British Columbia , Canada What is the role of cytoreductive surgery for recurrent ovarian cancer? • Surgery may be appropriate in selected patients. • As yet, there is no level I evidence that demonstrates a survival advantage associated with surgical cytoreduction for women with recurrent ovarian cancer • Cytoreductive surgery for women with recurrent ovarian cancer may be beneficial if it results in optimal cytoreduction as defined in A5 (A5 = optimal resection defined as macroscopic complete resection) •Randomized phase III trials evaluating the role of surgery in recurrent ovarian cancer are a priority 4th Ovarian Cancer Consensus Conference June 25 – 27, 2010 Vancouver, British Columbia , Canada What is the role of cytoreductive surgery for recurrent ovarian cancer? 1 0,9 0,8 survival probability 0,7 may be appropriate in selected • Surgery no residuals median OS 45.2 mos. patients. 0,6 • As yet, there is no level I evidence that demonstrates a survival 0,5 advantage associated with surgical cytoreduction for women with 0,4 recurrent ovarian cancer 0,3 residualscancer > 10 mmmay be • Cytoreductive surgery for women with recurrent ovarian 0,2 beneficial in A5 0,1 if it results in optimal cytoreduction as defined residuals 1 - 10 mm median OS 19.6 mos. (A5 = optimal resection defined as macroscopic complete resection) 0 0 12 24 36 48 •Randomized phase III trials evaluating the role of surgery in months Harter P et al. Ann Surg Oncol 2006 DESKTOP OVAR I recurrent ovarian cancer are a priority Surgical trial in platinumsensitive relapse (1) GOG 213 Intituive patient selection Surgical trial in platinumsensitive relapse (2) AGO-OVAR DESKSTOP III Selection on AGO score PS=0, 1st surgery residue =0, Ascite < 500cc R A N D O M Cytoreductive surgery N=408 no surgery platinum-based chemotherapy recommended Primary objective: OS March 2015 ACCRUAL COMPLETED! CHEMOTHERAPY 4th Ovarian Cancer Consensus Conference June 25–27, 2010 UBC Life Sciences Institute, Vancouver, BC Recurrent Ovarian Cancer: Population characteristics Platinum-Free Interval (Interval from last date of platinum dose until progression) Expected Platinum Sensitivity Progression while receiving last line of platinumbased therapy or within 1 month of last platinum dose Refractory 1-6 months Resistant 6-12 months Partially sensitive >12 months Fully sensitive 1000 100 900 90 800 80 700 70 600 60 500 50 400 40 300 30 200 20 100 10 0-3 Prog 0-3 Non PD 3-12 mos 12-18 mos Percentage Days Platinum-Free Interval and Survival 18+ mos PFS (days) 90 176 174 275 339 OS (days) 217 375 375 657 957 Response (%) 9 24 35 52 62 Pujade-Lauraine, Proc ASCO #829, 2002 Recommended guidelines for chemotherapy in relapse Platinum resistant Partially Platinum sensitive Fully Platinum sensitive Platinum-free interval <6 months 6-12 months >12 months Combination chemotherapy: Carboplatin combination: Platinum-based or trabectedin-PLD PLD, paclitaxel, ge mcitabine Non-platinum single agent: PLD, wkl paclitaxel, gemcita bine, topotecan PLD: pegylated liposomal doxorubicin Phase III Trials of Single Agent Chemotherapy PLD, Paclitaxel, Topotecan, Gemcitabine Drug A Drug B N TTP, weeks P OS, weeks P Comment Topotecan Paclitaxel 226 23 vs 14 NS 61 vs 43 NS 50% Crossover Paclitaxel (bolus) Paclitaxel (weekly) 208 38 vs 26 NS 34 vs 59 NS Less toxicity with weekly Oxaliplatin Paclitaxel 86 12 vs 14 NS 42 vs 37 NS 74% platinum resistant PLD Topotecan 481 16 vs 17 NS 60 vs 57 NS 54% platinum resistant; OS benefit in platinum sensitive subgroup. PLD Paclitaxel 214 22 vs 22 NS 46 vs 56 NS All patients taxane-naïve PLD Gemcitabine 195 16 vs 13 NS 59 vs 55 NS PLD Gemcitabine 153 16 vs 20 NS 55 vs 50 NS 56% platinum resistant Topotecan Treosulfan 357 22 vs 12 .001 56 vs 48 .02 Second-line / third-line therapy PLD or Topotecan Canfosfamide 461 19 vs 9 <.01 59 vs 37 <.0001 ASSIST-1 trial All third-line TTP, time to progression; OS, overall survival, PLD: pegylated liposomal doxorubicin Carboplatin-PLD versus Carboplatin-paclitaxel (CALYPSO) Median PFS, mo HR (95% CI) CD CP 11.3 9.4 0.82 (0.72, 0.94) Carbo-PLD less toxic than carbo-paclitaxel PFS Pujade-Lauraine E et al. J Clin Oncol 2010 1.00 Strategies to prolong PFI 1- Wait for symptoms Proportion surviving 0.25 0.50 0.75 • Overall survival Early Delayed Early (CA125 doubling) vs Delayed chemotherapy (at symptom) 0.00 Median Time with “good health score” 0 6 12 18 24 30 36 42 48 54 60 Months since randomisation HR=1.00 (95%CI 0.82-1.22) p=0.98 Early 7.1 months Delayed 9.2 months p=0.15 Rustin GJ, et al. Lancet 2010 Standard for patients with asymptomatic rise of CA125 • Observation • Tamoxifen Strategies to prolong platinum-free interval • Administer a non-platinum therapy 8 mos 5 mos relapse relapse CARBOPLATINBASED Cx Non-platinum therapy CARBOPLATINBASED Cx Strategies to prolong platinum-free interval MITO 8 • Administer a non-platinum therapy Recurrent 8 mos 5 mos OC 6-12 mos relapse relapse PLD 40 mg/m2 Q 28 d R CARBOPLATINBASED Cx Non-platinum therapy Paclitaxel 175 mg/m2 CARBOPLATINCarboplatin AUC = 5 BASED Cx Q 21 d Change to opposite treatment after disease progression Strategies to prolong platinum-free interval MITO 8 • Administer a non-platinum therapy Recurrent 8 mos 5 mos OC 6-12 mos relapse relapse PLD 40 mg/m2 Q 28 d R CARBOPLATINBASED Cx Non-platinum therapy Paclitaxel 175 mg/m2 CARBOPLATINCarboplatin AUC = 5 BASED Cx Q 21 d Change to opposite treatment after disease progression PFI is not the only prognostic factor for PFS in platinum-sensitive disease Nomogram Lee Cet al. Brit J Cancer 2011, 1-7 CHEMOTHERAPY Lurbinectedin (PM01183) is a novel synthetic entity, structurally related to trabectedin Platinum Resistant 1.0 PM01183 Topotecan Cumulative probability 0.9 (N=17 C=4) (N (N=16 C=2) 0.8 Lurbinectedin 0.7 0.6 HR: 0.30 p=0.005* - 5.7 mo. 0.5 1.7 mo. 0.4 0.3 0.2 0.1 0.0 0 1 2 3 4 5 6 7 8 9 10 Time ( months) months Presented by:A. Poveda ASCO 2014 11 12 13 14 15 16 TARGETED THERAPY Bevacizumab VEGF Bevacizumab • Monoclonal antibody • Binds VEGF-A Platinum-sensitive relapse 1°line chemotherapy CA-125 Surgery PFI: 12 months PFI, platinum-free interval Platinumsensitive relapse Platinum-sensitive relapse 1°line chemotherapy CA-125 Surgery PFI: 12 months PFI, platinum-free interval Platinumsensitive relapse Carbo-Gem Platinum-sensitive relapse 1°line chemotherapy CA-125 Surgery PFI: 12 months PFI, platinum-free interval Platinumsensitive relapse Platinum-sensitive relapse 1°line Platinumsensitive relapse chemotherapy CA-125 Surgery PFI: 12 months PFI, platinum-free interval 8 months Platinum-sensitive relapse 1°line Platinumsensitive relapse chemotherapy CA-125 Surgery PFI: 12 months PFI, platinum-free interval 8 months Platinum-sensitive relapse 1°line Platinumsensitive relapse chemotherapy CA-125 Surgery Bevacizumab, in combination with carboplatin and gemcitabine, is indicated 8for treatment of adult patients with months PFI: 12 months first recurrence of platinum-sensitive epithelianovarian, fallopian-tube or primary peritoneal cancer who have not received prior therapy with bevacizumab or other VEGF PFI, platinum-free interval inhibitors or VEGF-receptor-targeted agents Platinum-sensitive relapse 1°line chemotherapy CA-125 Surgery BEVACIZUMAB PFI: 12 months PFI, platinum-free interval Platinumsensitive relapse Platinum-sensitive relapse 1°line chemotherapy CA-125 Surgery BEVACIZUMAB PFI: 12 months PFI, platinum-free interval Platinumsensitive relapse Platinum-sensitive relapse 1°line Platinumsensitive relapse chemotherapy CA-125 Surgery BEVACIZUMAB Bevacizumab, in combination with carboplatin and gemcitabine, is indicated for treatment of adult patients with PFI: 12 months first recurrence of platinum-sensitive epithelianovarian, fallopian-tube or primary peritoneal cancer who have not received prior therapy with bevacizumab or PFI, platinum-free interval inhibitors or VEGF-receptor-targeted agents other VEGF Platinum-resistant relapse 1°line Platinumsensitive relapse Platinum resistant relapse Single agent CA-125 Surgery Bevacizumab in combination with paclitaxel, topotecan, or pegylated liposomal doxorubicin is indicated for the treatment of adult patients 4 months PFI: 12 months with platinum-resistant recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who received no twotwo prior nomore morethan than prior chemotherapy regimens and who havehave not not received prior chemotherapy regimens and who received priortherapy therapy with bevacizumab or VEGF inhibitor or receptor–targeted agents with bevacizumab or VEGF inhibitors or VEGF receptor–targeted agents Limitations to Bevacizumab use in relapse • Prior treatment with Bev • More than one prior line in platinum-sensitive disease and more than 2 in resistant • contraindications to BEV: uncontroled HTA, renal or cardiac function impairment, recent history of bleeding, thrombosis, wound healing trouble, bowel/bladder wall involvement Is platinum-free interval predictive of bevacizumab efficacy in relapsing OC ? Bevacizumab PFS efficacy in different OC subsets OCEANS3 AURELIA4 Tumor size/stage Platinumsensitive relapse with measurable disease Platinumresistant relapse with measurable disease in 80% Stratified Hazard Ratio 0.48 0.38 Absolute benefit in months 4.0 3.3 3. Aghajanian C, et al. J Clin Oncol. 2012;30(17):2039-2045. 4. Pujade-Lauraine E, et al. J Clin Oncol. 2014;32(13):1302-8 Bevacizumab PFS efficacy in different OC subsets ICON71 Low risk group Tumor size/stage Hazard ratio Absolute benefit in months GOG2182 Complete Stage III surgical with resection + macroscop stage III ic residue + with residue stage IV <1 cm ICON71 High risk group OCEANS3 AURELIA4 Stage III with residue >1 cm + stage IV Platinumsensitive relapse with measurable disease Platinumresistant relapse with measurable disease in 80% 0.87 0.72 0.67 0.48 0.38 <1 3.8 5.5 4.0 3.3 1. Perren TJ, et al. N Engl J Med. 2011;365(26):2484-2496. 2. Burger RA, et al. N Engl J Med. 2011;365(26):2473-2483. 3. Aghajanian C, et al. J Clin Oncol. 2012;30(17):2039-2045. 4. Pujade-Lauraine E, et al. J Clin Oncol. 2014;32(13):1302-8. Shall we wait for BEV administration until the disease get chemo- resistant? QoL improvement in AURELIA trial resistant disease –5.7 (–10.7 to – 0.7) –7.5 (–13.8 to – 1.2) –5.2 (–13.4 to 2.9) –7.3 (–16.9 to 2.3) –6.4 (–11.6 to – 1.3) Worsening Chemo (N=182) Improvement BEV + Chemo (N=179) Mixed Model Repeated Measures analysis (abdominal/GI symptoms) Clinical benefit in patients with ascites (n=113) Paracentesis in subgroup with ascites Primary hypothesis : improvement in abdominal/GI symptoms (≥15%) Patients (%) Responders: 44.0% vs 4.1% 39.9% difference [95% CI 23.9–55.9]). Cycle number Toxicity of interest during bevacizumab treatment in first-line (GOG218 & ICON7 trials) and in relapse (OCEANS & AURELIA trials) Adverse event n (%) GI events Hypertension GOG218 ICON7 2.6 a 3b OCEANS AURELIA 2.4c 4.4d 22.9 (gr≥2) 18 (gr≥3) 17.4 (gr≥3) 20 (gr≥2) Proteinuria (grade ≥3) 1.6 <1 8.5 1.7 Thromboembolic evente 7.4 8 6.8 5.0 Bleeding (grade ≥3) 2.4 1 6.5 1.1 PRES 0.2 0 1 0.6 PRES = posterior reversible encephalopathy syndrome; gr : grade; aperforation, fistula, necrosis and leak grade≥2;bperforation, fistula, abcess and wound-healing complications grade ≥3;c perforation, fistula and abcess all grades, wound-healing complications grade≥3; d perforation and fistula/abcess grade ≥2; earterial any grade, venous grade ≥3 OS according to crossover to BEV monotherapy in the CT arm Chemotherapy PD BEV 15 mg/kg q3w + chemotherapy PD 40% BEV 15 mg/kg q3wb (optional) R 1:1 Investigator’s choice (without BEV) CT alone arm Median OS, months (95% CI) No switch to BEV monotherapy (N=110) Switch to BEV monotherap y (N=72) BEV-CT arm (n=179) 11.3 (7.5–13.3) 17.2 (15.0–20.2) 16.6 (13.7–19.0) Unsolved questions Reuse of BEV in relapse after prior BEV treatment? Best cytotoxic drug to combine with BEV? Bevacizumab use in platinumsensitive relapse after Bev: MITO16MANGO ov2 Carboplatin combo PREVIOUS BEVACIZUMAB Carboplatin combo + BEVACIZUMAB OCEANS versus CALYPSO + BEV regimen:Platinum-sensitive AGOOVAR 2.21 trial platinumsensitive PREVIOUS ANTI-ANGIOGENIC AGENT (yes vs no) Bevacizumab with carboplatinpaclitaxel in platinum-sensitive relapse: GOG-0213 PACLITAX EL PACLITAX +EL BEVACIZUMAB + BEVACIZUMAB BEV efficacy in resistant patients PFS Chemo PFS BEV + chemo Topotecan 2.1 5.8 PLD 3.5 5.4 Paclitaxel 3.9 10.4 (weekly) Poveda A et al. ESMO 2012 BEV efficacy in resistant patients PFS Chemo PFS BEV + chemo OS Chemo OS BEV + chemo Topotecan 2.1 5.8 13.3 13.8 PLD 3.5 5.4 14.1 13.7 Paclitaxel 3.9 10.4 13.2 22.4 (weekly) Poveda A et al. ESMO 2012 Conclusion • Bevacizumab is an active drug in recurrent OC • Efficacy is not linked to platinum-free interval which makes BEV attractive for the treatment of resistant disease, particularly when symptomatic (ascites) • The best single cytotoxic drug/combination as BEV companion is under investigation • Criteria which could select patients who could benefit of Avastin reuse are eagerly Active anti-angiogenic drugs in recurrent ovarian cancer Antiangiogenic Setting drug Pazopanib resistant Trebananib < 12 months Fostrabulin Cediranib resistant Design HR (95%CI) Targets wkl paclitaxel + pazopanib VEGFR; PDGFR; c-kit; (0.25-0.69) FGFR wkl paclitaxel + pazopanib 0.66 Angio1 &2 (0.57–0.77) Bevacizumab + fostrabulin 0.42 0.67 Chemo + concurrent and 0.57 sensitive maintenance cediranib (0.44–0.74) Vascular disrupting agent VEGFR; PDGFR; FGFR Olaparib Anti-PARP olaparib • oral poly (ADP-ribose) polymerase inhibitor Study 19: Aim and design • Randomised, double-blind, placebo-controlled Phase II study Platinum-sensitive high-grade serous ovarian cancer > 6 months Platinum based chemotherapy relapse Maintenance Oral Olaparib <8 weeks Platinum based chemotherapy R 400 mg/bd 1:1 Treatment until disease progression Placebo bd Ledermann J et al. N Engl J Med 2012;366:1382–92 Study 19: Summary of endpoints in the BRCAm population 40 1. 0 0. 9 0. 8 0. 7 0. 6 0. 5 0. 4 0. 3 0. 2 0. 1 0 35 Proportion of patients progression-free +3 m 30 34.9 +8,6 m 25 20 +9,4 m Olaparib BRCAm 15 Placebo BRCAm +6,9 m 10 0 3 6 9 12 Time from randomisation (months) BRCAm (n=136) Events: total pts (%) Median PFS, months Olaparib Placebo 26:74 (35.1) 46:62 (74.2) 11.2 4.3 HR=0.18 95% CI: 0.11, 0.31; p<0.00001 15 15.6 31.9 23.8 15.2 11.2 5 4.3 6.2 0 initial Baseline relapse PFS1 Treatment Traitement traitement PFS1 Treatment rechute1 rechute Relapse1 Relapse 2 suivante (PFS2) (PFS2) OS Overall Survival APPROVAL “Monotherapy adult for the maintenance treatment of patients with platinum-sensitive relapsed BRCA-mutated (germline and/or somatic) high-grade serous epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in response (complete response or partial response) to platinum-based chemotherapy”. Olaparib for BRCAm high grade serous OC only? Frequency of germline BRCA mutation Total population Serous Endometrioid Clear Cell Mucinous Alsop et al 14.1% 16.6% 8.4% 6.3% NA Risch HA et al 13.2% 18.0% 5.8% 5.4% 5.4% 9.1% 0% Jacobi CE et al 13.9% 10.8% 0% 0% 0% Malander S et al 8% 7.6% 13.0% 12.5% 0% Soegaard M et al 7.1% 0% Alsop K, et al. J Clin Oncol 2012;30(21):2654‒2663.; Risch HA, et al. J Natl Cancer Inst 2006;98(3):1694‒1706. Soegaard M, et al. Clin Cancer Rev. 2008;14(12):3761-3767. Jacobi CE, et al. Genet Med 2007;9(3):173‒179; Malander S, et al. Eur J Cancer. 2004;40(3):422-428. Pennington KP et al Clin Cancer Res. 2014 February 1; 20(3): 764–775 Olaparib for BRCAm only? Platinum sensitivity and NonBRCA HRm genes Proportion of patients progression-free Olaparib and BRCA wt No of patients Platinum sensitivi ty BRCAm (somatic & germline) 67 85% Non-BRCA HRm genes 18 78% No HRm 158 60% Mutation (m) in Homologous recombination (HR) genes Olaparib BRCAwt Placebo BRCAwt 0 3 6 9 12 Time from randomisation (months) BRCAwt (n=118) Olaparib Placebo Events: total pts (%) 32:57 (56.1) 44:61 (72.1) Median PFS, months 5.6 5.5 15 HR=0.53 95% CI: 0.33, 0.84; p=0.007 Ledermann J et al. J Clin Oncol 2013;31(15S):abst 5505 Pennington KP et al. Clin Cancer Res 2015;20(3) 764 (%) Is platinum-free interval predictive of bevacizumab efficacy in relapsing OC ? Correlation Between Olaparib Response and Prior Platinum Sensitivity and BRCA mutation status Germline BRCA Status BRCA mutation positive1 BRCA mutation negative2 Response to Prior Platinum RECIST Response to Olaparib Platinum sensitive 6/13 (46%) Platinum resistant 8/24 (33%) Platinum sensitive 10/20 (50%) Platinum resistant 1/26 (4%) 1. Fong PC, et al. J Clin Oncol. 2010;28(15):2512-2519. 2. Gelmon KA, et al. Lancet Oncol. 2011;12(9):852-861. Olaparib Trial in Heavily Pretreated Ovarian Cancer • n = 137 pts with measurable disease, gBRCA+, and treated with at least 3 lines of prior therapy • Response rate: 34% (26-42) with a median response duration of 7.9 months • Conditional approval by FDA Kaufman B et al. J Clin Oncol. 2015;33(3):244-50. CONDITIONAL APPROVAL Lynparza is indicated as monotherapy in patients with deleterious germline BRCA mutated (as detected by an FDA-approved test) advanced ovarian cancer with 3 or more prior lines of chemotherapy Heterogeneity of drug label according to the continents Drug/indication EU Japan BEV first line X X BEV platinum-sensitive X X X X BEV platinum-resistant US X OLAPARIB platinum-sensitive OLAPARIB multiple lines X X And heterogeneity of reimbursement! Guideline for recurrent OC MODULATION FROM STANDARD FRAILTY HISTOLOGY Platinumfree interval Asymptomatic CA125 increase •follow-up or Tam PATIENT WISH GEOGRAPHY Label-Reimbursement Prior Bevacizumab Number of prior lines PLATINUM-SENSITIVE PFI>6 months BRCAm Multiple lines (>3) •Best of care or olaparib (BRCAm, US) PLATINUM-RESITANT PFI<6 months • Carboplatin-gemcitabine-bevacizumab (1st PS relapse, no prior BEV) • Platin-based chemo followed by olaparib maintenance (BRCAm) • Bevacizumab with wkl paclitaxel or PLD, topotecan (1st or 2nd relapse, no prior BEV) • • Carboplatin combination or nonplatinum combination (PFI 6-12,..) • Single non-platinum agent drug • BACK UP slides A Randomized Phase 2 Trial of Olaparib and Cediranib vs Olaparib Alone in Recurrent Platinum-sensitive Ovarian Olaparib Cancer capsules Dx platinumsensitive recurrent ovarian cancer 400mg BID Disease progression by RECIST v1.1 criteria Randomize 1:1 Cediranib 30mg daily + Olaparib capsules 200mg BID PFS events Median PFS NonHematologic Adverse Event Olaparib Ced/Ola (N = 46) (N = 44) Hypertension - 18 (41) Grade 3/4 Olaparib Ced/Olap 28 19 Diarrhea - 10 (23) 9.0 mo 17.7 mo Fatigue 5 (11) 12 (27) Nausea - 2 (5) p=0.005 HR 0.42 (95% CI: 0.23-0.76) Headache - Liu ASCO 22014 (5) Presented by: Joyce