Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
New developments in balance
medicine
Tim Price
Consultant ENT Surgeon
November 2011
Balance disorders
30% population consult on giddiness by age
65
Commonest reason for GP appointment in
the over 75’s
Early retirement/ chronic illness in 18%
5500 patients per year-Leicester Balance
Centre.
COMMON ENT CAUSES OF
BALANCE DYSFUNCTION
BPPV
Vestibular neuronitis/ Labyrinthitis
Meniere’s disease / syndrome
Migraineous Vertigo {Migraine-associated
Dizziness / Labyrinthine Migraine}
The most common cause of balance
disturbance.
Occurs in 5-8% of all cases of migraine
33% of cases have no headache
66% have no neurological deficit.
Mean age of onset 40 years.
Female :male ratio 2:1
Migrainous Vertigo symptoms
Vertigo / dysequilibrium / or both
Variable duration (sec to days)
Aural fullness (10%)
Hearing changes (6%)
Visual blurring (6%)
Bilateral tinnitus (5%)
Unilateral tinnitus (4%)
Symptoms continued
Bilateral ear pain (2%)
Unilateral ear pain (2%)
Diplopia (1%)
Hemianeasthesia (1%)
Differential diagnosis
Vestibular paroxysmia
Meniere’s disease
VBI
Vestibular epilepsy
Familial episodic ataxia
Pathophysiology
Uncertain
Genetic basis
Vascular spasm / Hypoperfusion
Neuronal hyperexcitability (calcium
channelopathy)
Trigger factors are important.
Management
Dietary {6 C’s}
Medication for both acute attacks and
prophylaxis
Include TCA’s / beta blockers etc.
Referral for specialist opinion.
Conclusions
Migraine related balance disturbance is
common
Can be difficult to diagnose.
High index of suspicion
Specialist opinion may be valuable.
Low dose TCA, beta-blockers and migraine
diets are well tolerated and efficacious.
BPPV
2ND
MOST COMMON CAUSE OF
VERTIGO.
Symptoms
Occurs with specific head movements.
Rolling over in bed.
May follow on from a minor head injury.
Symptoms very brief -fades after 30-60 seconds.
No hearing loss.
Spontaneous resolution in 3 to 6 months
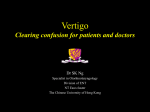
Detection / diagnosis:
Dix Hallpike Manoeuvre
Tests the posterior and anterior semi circular canals
Gravitational effect – produces circulation of endolymph - otoliths in one of the canals
produces drag
A few seconds latency and then symptom of intense vertigo with rotational, geotropic
nystagmus.
fades after 30-60 sec.
Repeatable but fatigable.
Treatment:
Epley manoeuvre
Labyrinthitis
Third most common cause of vertigo after
BPPV.
Characterized by sudden onset of severe
vertigo without associated hearing loss.
Usually completely remits within 6 months
Historical Synonyms
Epidemic vertigo (Charters 1957)
Neurolabyrinthitis epidermica
(Meulengracht 1950)
Acute labyrinthitis (Burrowes 1952)
Vestibular paralysis (Hart 1965)
Vestibular neuritis (Coats 1969)
Vestibular Neuritis
Bell’s Palsy
HSV 1 has been implicated in the etiology
Found virus in 60% of all vestibular ganglia
examined
Latent Herpes Simplex virus Type 1 in Human Vestibular Ganglia. Futura Y et
al Acta Otolaryngol Suppl. 503:85-89, 1993.
HSV-1 Geniculate and Vestibular Ganglia. Arbusow V et al Ann Neurol
46:3,416-419, 1999.
The beneficial effect of
Methylprednisolone in acute vestibular
vertigo
Ariyasu L et al Arch. Otolaryngology Head and Neck Surg 116:700703, 1990
20 patients
Placebo-controlled, blinded, randomized,
crossover study
9/10 steroid treated patients with significant
early reduction in vertigo.
3/10 placebo treated patients with
significant early reduction in vertigo.
Methylprednisolone, valacyclovir, or the
combination for Vestibular Neuritis
Strupp et al NEJM 351:4, 28-35, 2004
Prospective randomized double blinded trial
141 patients
4 limbs– placebo(38), antiviral (35), steroid (35),
steroid plus antiviral (35)
Analysis of caloric response recovery Day1 or 2
versus one year.
Significant steroid effect, no effect of antiviral
with or without steroid
Major flaw is late enrolement up to 3 days!
Where do we go from here?
Consider Vestibular Neuritis as a treatable
acute neuropathy
Steroid therapy has some literature support.
Randomized placebo-controlled doubleblinded trial with early enrollment.
Multicenter trial
Proposed therapy for Acute
vestibular Neuritis
Vestibular sedative (Stemetil)
IV/IM Dexamethasone 8mg
(hydrocortisone)
Oral Prednisolone
Acyclivir/ Famcyclovir.
And now for something
completely different!
“Doctor I feel a bit dizzy and I can hear my
eyes moving in my head”
“Doctor I can hear my foot steps in my head
when I walk”
“I can hear my voice in my head”
Superior Semicircular Canal
Dehiscence
Described in 1998 in:
Rare condition caused by a third window
into the inner ear.
Sound- and/or pressure-induced vertigo due
to bone dehiscence of the superior
semicircular canal.
Minor et al Archives Otolaryngology Head
Neck Surg. 1998 Mar; 124(3):249-58
Etiology
Signs and symptoms usually present during
adulthood, and half of patients report a
precipitating head injury.
Suggests two stage process:
1. Anomolous development of thin layer of bone
over SCC.
2. Second event (trauma or sudden change in
pressure) that fractures the thin bone or
destabilizes dura over the dehiscence.
(? 3. or slow erosion due to gravity/pulse
pressure.)
SCDS Symptoms
Autophony- hear the sound of their own
voice as a distubingly loud and distorted
sound deep in their heads.
Also hear creaking and cracking of joints,
sound of footsteps, chewing and digestive
noises,
eyeballs moving in their sockets like
sandpaper on wood.
SCDS- symptoms
Sound-induced loss of balance/ vertigo,
chronic disequilibrium or dizziness, caused
by the dysfunction of the superior
semicircular canal.
Tullio phenomenon nystagmus and oscillopsia.
SCDS- symptoms
Triggered by normal sounds
Theatre or music hall!
Change of pressure in the middle ear
(blowing nose or flying) can also cause
imbalance and a type of drop attack.
SCDS- symptoms
Hyperacusis- over-sensitivity to sound
Low frequency conductive hearing loss
Fullness of ear
Pulsatile tinnitis
Brain fog
Fatigue
SCDS- Examination
Low frequency conductive hearing loss
Vibrotactile 125Hz Tuning fork
Eye movements with sound, pressure
(ENG)
Differential Diagnosis
Meniere’s Disease
Perilymphatic fistula
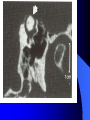
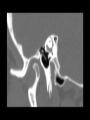
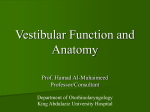
Investigations
CT Temporal bone
Fine cuts in the plane of the superior canal
(Oblique Sagittal reformats)
Vestibular evolked myogenic potentials
(VEMPS)- increased amplitude on testing.
Management
Reassurance
avoidance
Ear plug
surgery
Surgery
Conclusions
SCC dehiscence syndrome may be most
common cause of Tullio phenomenon.
Specific localizing signs
Treatable form of vestibular disease.
Diagnosis can be difficult without high
index of suspicion –often present with nonspecific “dizzy feeling”.
Any questions?