Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Learning Qualitative Models from
Physiological Signals
by
David Tak-Wai Hau
S.B., Massachusetts Institute of Technology (1992)
Submitted to the Department of Electrical Engineering and Computer Science
in partial fulfillment of the requirements for the degree of
Master of Science in Electrical Engineering and Computer Science
at the
MASSACHUSETTS INSTITUTE OF TECHNOLOGY
May 1994
(
David Tak-Wai Hau, MCMXCIV. All rights reserved.
The author hereby grants to MIT permission to reproduce and distribute publicly
paper and electronic copies of this thesis document in whole or in part, and to grant
others the right to do so.
Author
. ...........................
.
-.
Department of Electrical Engineering and Computer Science
May 17, 1994
Certified by ..................................................
( Eico
Project Manager, Hewlett-P
,~7o----~
Certified by ....................--
...-
...
W. Coiera
ard Laboratories
Thesis Supervisor
...-
Ror G. Mark
Grover Hermann Professor in Health Sciences and Technology
Cd
(x
Anen+
[~
ThesisSupervisor
W.,n
Accepteu Dy............
FredericR. Morgenthaler
tee on Graduate Students
LIBRARSES
Learning Qualitative Models from
Physiological Signals
by
David Tak-Wai Hau
Submitted to the Department of Electrical Engineering and Computer Science
on May 17, 1994, in partial fulfillment of the
requirements for the degree of
Master of Science in Electrical Engineering and Computer Science
Abstract
Physiological models represent a useful form of knowledge, but are both difficult and time
consuming to generate by hand. Further, most physiological systems are incompletely
understood. This thesis addresses these two issues with a system that learns qualitative
models from physiological signals. The qualitative representation of models allows incom-
plete knowledgeto be encapsulated, and is based on Kuipers' approach used in his QSIM
algorithm. The learning algorithm allows automatic generation of such models, and is based
on Coiera's GENMODEL algorithm. We first show that QSIM models are efficiently PAC
learnable from positive examples only, and that GENMODEL is an algorithm for efficiently
constructing a QSIM model consistent with a given set of examples, if one exists. We then
describe the learning system in detail, including the front-end processing and segmenting
stages that transform a signal into a set of qualitative states, and GENMODEL that uses
these qualitative states as positive examples to learn a QSIM model. Next we report re-
sults of experiments using the learning system on data segments obtained from six patients
during cardiac bypass surgery. Useful model constraints were obtained, representing both
general physiological knowledge and knowledge particular to the patient being monitored.
Model variation across time and across different levels of temporal abstraction and fault
tolerance is examined.
Thesis Supervisor: Enrico W. Coiera
Title: Project Manager, Hewlett-Packard Laboratories
Thesis Supervisor: Roger G. Mark
Title: Grover Hermann Professor in Health Sciences and Technology
Acknowledgements
First I would like to thank Enrico Coiera, my supervisor at HP Labs, for offering me an
extremely interesting project which combines my interests in artificial intelligence, signal
processing and medicine, and for being a really great supervisor. I especially thank him for
his superb guidance throughout the project, and for his encouragement and patience in the
write-up process.. It has been my pleasure to have him as a mentor and a friend.
I would also like to thank Dave Reynolds at HP Labs for offering me a lot of help and
advice in the project, and for reading part of a draft of the thesis. The overall front-end
processing scheme and the idea of using Gaussian filters came from him. I also appreciate
his excellent sense of humor. Every discussion with him has been a lot of fun.
I am grateful to Professor Roger Mark for taking time out of his busy schedule to
supervise my thesis. I thank him for his patience and his comments in the write-up process.
I really enjoyed the discussions with him in which I learned a lot about cardiovascular
iphysiology.
My friend David Maw kindly let me store my enormous number of data files in his server
at LCS. I thank him deeply for his help.
Most of all, I thank my family for their never-ending love and encouragement. I dedicate
this thesis to my mother.
This thesis describes work done while the author was a VI-A student at Hewlett-Packard
Laboratories, Bristol, U.K. in Spring and Summer 1993.
3
To my mother
4
Contents
1 Introduction
14
2 Qualitative Reasoning
17
2.1 Qualitative Model Constraints
........
17
2.2
Qualitative System Behavior.
19
2.3
Qualitative Simulation: QSIM.........
21
2.4
Learning Qualitative Models: GENMODEL .
21
2.5 An Example: The U-tube ...........
22
2.5.1 Qualitative Simulation of the U-tube .
24
2.5.2 Learning the U-tube Model ......
24
3 Learning Qualitative Models
28
...... .... . .28
3.1 Probably Approximately Correct Learning ........
3.1.1
Definitions.
3.1.2
PAC Learnability ..................
3.1.3
Proving PAC Learnability .............
3.1.4
An Occam Algorithm for Learning Conjunctions
. ...
3.2 The GENMODEL Algorithm ...............
3.3
3.4
QSIM Models are PAC Learnable .............
3.3.1
The Class of QSIM Models is Polynomial-Sized .
3.3.2
QSIM Models are Polynomial-Time Identifiable
GENMODEL ........................
3.4.1
Dimensional Analysis.
3.4.2
Performance on Learning the U-Tube Model
3.4.3
Version Space ....................
5
.......... . .28
.......... . .29
.......... . .32
.......... . .33
.......... . .35
.......... . .35
.......... . .35
.......... . .37
.......... . .37
.......... . .38
.......... . .38
. .
...
...
.
.30
3.5
3.4.4
Fault Tolerance ...........................
39
3.4.5
Comparison of GENMODEL with Other Learning Approaches
40
Applicability of PAC Learning
......................
4 Physiological Signals and Mode
4.1
4.2
4.1.1
Primary Measurements
4.1.2
Derived Values ....
A Qualitative
Cardiovascular
5 System Architecture
5.1
Overvievw .
5.2 Front-End System ......
5.2.1 Artifact Filter.....
5.2.2
Median Filter.
5.2.3
Temporal Abstraction
5.2.4 Gaussian Filter ....
5.3
......................
......................
......................
......................
Hemodynamic Monitoring
5.2.5
Differentiator.
5.2.6
An Example.
Segmenter ...........
I
..........................
..........................
..........................
..........................
..........................
..........................
..........................
..........................
..........................
6 Results and Interpretation
6.1
6.2
Inter-Patient
Model Comparison:
42
44
44
44
46
49
54
54
54
56
57
57
60
66
68
68
72
Patients
73
1
.5 . . . . . . . . . . . . . . . ..
6.1.1
Patient 1 .
. . . . .
73
6.1.2
Patient 2 .........
. . . . .
80
6.1.3
Patient 3 .........
. . . . .
87
6.1.4
Patient 4 .........
. . . . .
94
6.1.5
Patient 5 .........
. . . . .
Intra-Patient
Model Comparison: Patient
,Sement
1-6..........
6,
101
108
6.2.1 Segment
i .........
. . . . . Se me t . 1-6.. . . . . . . . . . .
108
6.2.2
Segment 2 .........
. . . . . . . . . . . . . . . . . . . . . .
115
6.2.3
Segment 3 .........
. . . . .
122
6.2.4
Segment 4 .........
. . . . .
131
6
6.2.5
Segment 5 .................................
138
6.2.6
Segment 6 .................................
145
7 Discussion
7.1
7.2
152
Validity of Models Learned
. . . . . . . . . . . . . . . .
.
........
7.1.1
Model Variation Across Time ......................
153
7.1.2
Model Variation Across Different Levels of Temporal Abstraction . .
153
7.1.3
Model Variation Across Different Levels of Fault Tolerance
154
7.1.4
Sources of Error
.....
.............................
Applicability in Diagnostic Patient Monitoring
155
................
156
7.2.1
A Learning-Based Approach to Diagnostic Patient Monitoring
7.2.2
Generating Diagnoses Based on Models Learned
.
..........
8 Conclusion and Future Work
8.1
152
Future Work
8.1.1
.
156
157
159
...................................
160
IJsing Corresponding Values in Noisy Learning Data .........
.Bibliography
160
165
7
List of Figures
2-1
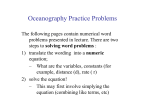
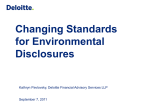
Qualitative reasoning is an abstraction of mathematical reasoning with differential equations and continuously differentiable functions
2-2
..........
Qualitative states following addition of an increment of fluid to one arm of a
U-tube....................................
2-3
2-4
18
...
22
Prolog representation for the U-tube model, initialized for an increment of
fluid added to arm a ................................
23
Qualitative model of a U-tube.
24
..........................
2-5 Output of the system behavior generated by running QSIM on the U-tube
model
...................
2-6
.....................
25
Qualitative plots for the qualitative states of a U-tube following addition of
an increment of fluid to one arm until equilibrium is reached. ........
2-7
26
Output of the U-tube model generated by GENMODEL on the given behavior. Note that the model learned is the same as the original model shown
previously ......................................
3-1 GENMODEL algorithm
27
..............................
34
3-2 Using the upper and lower boundary sets to represent the version space...
39
3-3 GENMODEL algorithm with fault tolerance.
40
.................
4-1 Deriving the systolic, diastolic and mean pressures from the arterial blood
pressure waveform .................................
45
4-2 Deriving the stroke volume from the arterial blood pressure waveform....
47
4-3 Cardiac output curves for the normal heart and for hypo- and hypereffective
hearts................................
.........
5-1 Overall architecture of the learning system.
8
..................
50
54
5-2 Architecture used for front-end processing of physiological signals.
.....
55
5-3 An artifact found in blood pressure signals, caused by flushing the blood
pressure line with high pressure saline solution
5-4
.................
56
An artifact found in blood pressure signals, caused by blood sampling from
the blood pressure catheter ...........................
5-5
56
A general artifact caused by the transducer being left open to air.
.....
57
5-6 The median filter removes features with durations less than half of its window
length, but retains sharp edges of remaining features ..............
5-7
The effect of aliasing in the segmentation of a signal with the temporal ab-
straction parameter set to
T.
g(t) is aliased into h(t) in the qualitative be-
havior produced ...........
5-8
58
.......................
Plot of the Hanning window wn].
61
........................
64
5-9 Plots of impulse responses h[n] of Gaussian filters for a = 20,40, 60,80, 100.
64
5-10 Plots of frequency responses H(Q) of Gaussian filters for a = 20, 40, 60, 80, 100. 65
5-11 Impulse response of an FIR bandlimited differentiator
.............
5-12 Frequency response of an FIR bandlimited differentiator ............
66
67
5-13 Equivalent frequency responses of a Gaussian filter in cascade with a bandlimited differentiator for a = 20, 40, 60, 80, 100 .................
67
5-14 A segment of the mean arterial blood pressure (ABPM) signal. Note the
artifacts at t = 600, 1000, 3400 seconds.
.....................
68
5-15 The ABPM data segment processed by the artifact filter. Note that the
artifacts have been filtered but the signal contains many impulsive features.
68
5-16 The ABPM data segment processed by the median filter. Note that the
impulsive features have been filtered
.......................
69
5-17 The ABPM data segment processed by the Gaussian filter. Note that the
signal has been smoothed
............................
5-18 The ABPM data segment processed by the differentiator.
69
..........
69
5-19 Overall scheme of segmentation to produce a qualitative behavior from processed signals and derivatives ..........................
6-1 Patient
70
: Original Signals. Note the relatively constant heart rate due to
the effect of beta-blockers
............................
9
73
6-2 Patient 1: Filtered Signals (L = 61)
74
6-3 Patient 1: Filtered Signals (L = 121) . . . . . . . . . . . . . . . . . . . . . .
75
6-4 Patient 1: Filtered Signals (L = 241)
. . . . . . . . . . . ..
76
6-5 Patient 1: Filtered Signals (L = 361)
. . . . . . . . . . . . . . . . . . . . .
77
6-6 Patient 1: Filtered Signals (L = 481)
. . . . . . . . . . . . . . . . . . . . .
78
6-7 Patient 1: Filtered Signals (L = 601)
..............
79
......
. . . . .
. . .....
. ...
6-8 Patient 2: Original Signals. Note the relatively constant heart rate due to
artificial pacing ..............
. . . . . . . . . . . . . . . .
80
6-9 Patient 2: Filtered Signals (L = 61)
. . . . . . . . . . . . . . . .
81
6-10 Patient 2: Filtered Signals (L = 121)
. . . . . . . . . . . . . . . .
82
6-11 Patient 2: Filtered Signals (L = 241)
. . . . . . . . . . . . . . . .
83
6-12 Patient 2: Filtered Signals (L = 361)
. . . . . . . . . . . . . . . .
6-13 Patient 2: Filtered Signals (L = 481)
. . . . . . . . . . . . . . . .
85
6-14 Patient 2: Filtered Signals (L = 601) .
. . . . . . . . . . . . . . . .
86
6-15 Patient :3: Original Signals .......
. . . . . . . . . . . . . . . .
6-16 Patient 3: Filtered Signals (L = 61)
. . . . . . . . . . . . . . . .
88
6-17 Patient :3: Filtered Signals (L = 121)
. . . . . . . . . . . . . . . .
89
6-18 Patient 3: Filtered Signals (L = 241)
. . . . . . . . . . . . . . . .
90
6-19 Patient 3: Filtered Signals (L = 361)
. . . . . . . . . . . . . . . .
91
6-20 Patient 3: Filtered Signals (L = 481)
. . . . . . . . . . . . . . . .
92
. . . . . . . . . . . . . . . .
93
6-21 Patient :3: Filtered Signals (L = 601) .
.
.
.
.
.
.84
.87
6-22 Patient 4: Original Signals. Note the relatively constant heart rate due to
the effect of beta-blockers
......
94
6-23 Patient 4: Filtered Signals (L = 61). Note that the trends of the relatively
constant heart rate are amplified. ..
. . . . . . . . . . . . . .
95
6-24 Patient 4: Filtered Signals (L = 121)
. . . . . . . . . . . . . .
96
6-25 Patient 4: Filtered Signals (L = 241)
. . . . . . . . . . . . . .
97
6-26 Patient 4: Filtered Signals (L = 361)
. . . . . . . . . . . . . .
98
6-27 Patient 4: Filtered Signals (L = 481)
. . . . . . . . . . . . . .
99
6-28 Patient 4: Filtered Signals (L = 601)
. . . . . . . . . . . . . . . 100
6-29 Patient 5: Original Signals. Note the relatively constant heart rate due to
the effect of beta-blockers ......................
10
101
6-30 Patient 5: Filtered Signals (L = 61). Note that the trends of the relatively
constant heart rate are amplified .
. . . . . . . . . . . . . . . . 102
6-31 Patient
5:
Filtered Signals (L = 121)
. . . . . . . . . . . . . . . . 103
6-32 Patient
5:
Filtered Signals (L = 241)
. . . . . . . . . . . . . . . .104
6-33 Patient
5: Filtered Signals (L = 361)
. . . . . . . . . . . . . . . .105
6-34 Patient
5: Filtered Signals (L = 481)
. . . . . . . . . . . . . . . . 106
6-35 Patient
5:
Filtered Signals (L = 601)
. . . . . . . . . . . . . . . ..107
6-36 Patient 6, Segment 1: Original Signals
.
. . . . . . . . . . . . . . . . 108
1: Filtered Signals (1 = 61)
. . . . . . . . . . . . . . . . 109
6-38 Patient 6, Segment
1: Filtered Signals (1L = 121)
. . . . . . . . . . . . . . . ..110
6-39 Patient 6, Segment
1: Filtered Signals (1L = 241)
. . . . . . . . . . . . . . .
6-40 Patient
6, Segment
1: Filtered Signals (1L = 361)
. . . . . . . . . . . . . . . . 112
6-41 Patient 6, Segment
1: Filtered Signals (1L = 481)
. . . . . . . . . . . . . . . . 113
6-42 Patient 6, Segment 1: Filtered Signals (1L = 601)
. . . . . . . . . . . . . . . . 114
6-43 Patient 6, Segment 2: Original Signals .
. . . . . . . . . . . . . . . . 115
6-44 Patient 6, Segment
2: Filtered Signals (L = 61)
. . . . . . . . . . . . . . . . 116
6-45 Patient 6, Segment
2:
Filtered Signals (L = 121) . . . . . . . . . . . . . . . ..117
6-46 Patient 6, Segment
2:
Filtered Signals (L = 241) . . . . . . . . . . . . . . . . 118
6-47 Patient 6, Segment
2:
Filtered Signals (L = 361) . . . . . . . . . . . . . . . . 119
6-48 Patient 6, Segment
2:
Filtered Signals (L = 481) . . . . . . . . . . . . . . . ..120
6-49 Patient 6, Segment
2: Filtered Signals (L = 601)
. . . . . . . . . . . . . . . . 121
6-50 Patient 6, Segment
3: Original Signals ......
. . . . . . . . . . . . . . . . 122
6-51 Patient 6, Segment
3:
6-37 Patient
6, Segment
Filtered Signals (L = 61)
l...111
. . . . . . . . . . . . . . . . 123
6, Segment 3:
Filtered Signals (L = 121) . . . . . . . . . . . . . . . ..124
6-53 Patient 6, Segment 3:
Filtered Signals (L = 241) . . . . . . . . . . . . . . . . 125
6-54 Patient
6, Segment 3:
Filtered Signals (L = 361) . . . . . . . . . . . . . . . . 126
6-55 Patient
6, Segment 3:
Filtered Signals (L = 481) . . . . . . . . . . . . . . . . 127
6-56 Patient
6, Segment 3: Filtered Signals (L = 601) . . . . . . . . . . . . . . .
6-57 Patient
6, Segment 4: Original Signals ......
. . . . . . . . . . . . . . . . 131
6-58 Patient
6, Segment 4: Filtered Signals (L = 61)
. . . . . . . . . . . . . . . . 132
6-59 Patient
6, Segment 4: Filtered Signals (L = 121) . . . . . . . . . . . . . . . . 133
6-52 Patient
6-60 Patient 6, Segment 4: Filtered Signals (L = 241)
11
...
.....
.129
134
6-61 Patient
6, Segment 4:
Filtered Signals (L = 361) . . . . . . . . . . . . . . . . 135
6-62 Patient
6, Segment 4:
Filtered Signals (L = 481) . . . . . . . . . . . . . . . . 136
6-63 Patient
6, Segment 4:
Filtered Signals (L = 601) . . . . . . . . . . . . . . .
6-64 Patient
6, Segment 5: Original Signals ......
6-65 Patient
6, Segment 5:
Filtered Signals (L = 61)
6-66 Patient
6, Segment 5:
Filtered Signals (L = 121)
6-67 Patient
6, Segment 5:
Filtered Signals (L = 241)
6-68 Patient
6, Segment 5:
Filtered Signals (L = 361) . . . . . . . . . . . . . . . . 142
6-69 Patient
6, Segment 5: Filtered Signals (L = 481)
. . . . . . . . . . . . . . .
.143
6-70 Patient
6, Segment 5: Filtered Signals (L = 601)
. . . . . . . . . . . . . . .
.144
6-71 Patient
6, Segment 6: Original Signals ......
. . . . . . . . . . . . . . . . 145
6-72 Patient
6, Segment 6:
Filtered Signals (L = 61)
6-73 Patient
6, Segment 6:
Filtered Signals (L = 121) . . . . . . . . . . . . . . .
6-74 Patient
6, Segment 6:
Filtered Signals (L = 241) . . . . . . . . . . . . . . . . 148
6-75 Patient
6, Segment 6: Filtered Signals (L = 361) . . . . . . . . . . . . . . . . 149
6-76 Patient
6, Segment 6: Filtered Signals (L = 481) . . . . . . . . . . . . . . .
.137
. . . . . . . . . . . . . . . . 138
. . . . . . . . . . . . . . .
.139
......... ...... ....
141
.................... 140
. . . . . . . . . . . . . . . . 146
.147
.150
6-77 Patient 6, Segment 6: Filtered Signals (L = 601) . . . . . . . . . . . . . . . . 151
7-1 Two approaches to diagnostic patient monitoring. In the learning-based approach, models are continually learned from the patient data. In the historybased approach, a hypothesize-test-refine cycle is used to generate models
that best match the patient data.
based on the current model.
In each approach, diagnoses are made
...........................
157
8-1 The two functions a and b shown obey direction-of-change consistency for
the qualitative constraint M+ (a, b), but not magnitude consistency......
162
8-2 Incorporating intervals into corresponding value sets is analogous to adding
a bounding envelope to monotonic functions .................
12
164
List of Tables
5.1
Table showing the orders M and lengths L of the Gaussian filters corresponding to a = 10, 20, 40, 60, 80, 100. . . . . . . . . . . . . . . .
13
.
......
65
Chapter
1
Introduction
Physiological models represent a useful form of knowledge because they encapsulate structural information of the system and allow deep forms of reasoning techniques to be applied.
For example, such models are used in many prototype intelligent monitoring systems and
medical expert systems. However, generating physiological models by hand is difficult and
time consuming. Further, most physiological systems are incompletely understood. These
factors have hindered the development of model-based reasoning systems for clinical decision
support.
Qualitative models permit useful representations of a system to be developed in the
absence of extensive knowledge of the system. In the medical domain, such models have
been applied to:
* diagnostic patient monitoring of acid-base balance [6]
* qualitative simulation of the iron metabolism mechanism [14]
* qualitative simulation of urea extraction during dialysis [2]
* qualitative simulation of the water balance mechanism and its disorders [19]
* qualitative simulation of the mechanism for regulation of blood pressure [19]
Further, recent developments in the machine learning community have produced methods
of automatically inducing qualitative models from system behaviors. Applying such techniques to learning physiological models should not only benefit knowledge acquisition, but
also provide a useful tool for physiologists who need to process vast amounts of data and
14
induce useful theoretical models of the systems they study. The learning system could also
serve as a tool for model-based diagnosis. For example, it could be incorporated into a
diagnostic patient monitoring system to perform adaptive model construction for diagnosis
in a dynamic environment.
In this thesis, we describe a system for learning qualitative models from physiological
signals. The qualitative representation of physiological models used is based on Kuipers'
approach, used in his qualitative simulation system QSIM [20]. The learning algorithm
adopted is based on Coiera's GENMODEL system described in [5].
There has been much work in the machine learning community on learning qualitative
models from system behaviors [4, 38, 28]. However, most of these efforts involve learning
from ready-made qualitative behaviors, or at best simulated quantitative data only. Few,
if any, address the issues of learning qualitative models from real, noisy data. Yet such
domains are precisely ones where incomplete information prevails, and where automatic
generation of qualitative models is most useful. This thesis addresses such a need with
a learning system that constructs qualitative models from physiological signals, which are
often corrupted with artifacts and other kinds of noise.
In our system, we use signals derived from hemodynamic measurements, including:
* heart rate (HR)
* stroke volume (SV)
* cardiac output (CO)
* mean arterial blood pressure (ABPM)
* mean central venous pressure (CVPM)
* ventricular contractility (VC)
* rate pressure product (RPP)
* skin-to-core temperature gradient (AT)
The thesis is organized into the following chapters:
Chapter 2 provides an overview of qualitative reasoning, with focus on qualitative simulation, learning qualitative models, and the relationship between these two tasks. The
classic example of the U-tube model is discussed, showing the sequence of qualitative
states obtained by running QSIM on the model, and the result of using GENMODEL
to learn the original model from these states.
15
Chapter 3 analyzes the learnability of qualitative models. QSIM models are shown to
be PAC learnable from positive examples only, and GENMODEL is shown to be an
algorithm for efficiently constructing a QSIM model consistent with a given set of
examples, if one exists. The GENMODEL algorithm and the newly added features of
dimensional analysis and fault tolerance are discussed in detail. The chapter ends with
a comparison of GENMODEL with other approaches of learning qualitative models,
and a discussion of difficulties of applying the PAC learning algorithm to learning
qualitative models from physiological signals.
Chapter 4 describes the various signals from hemodynamic monitoring used for our learning experiments. A qualitative model of the human cardiovascular system using these
signals is provided as a 'gold standard' model, representing the author's best estimate
of the target concepts learnable from the data.
Chapter 5 discusses the architecture of the learning system in detail, with emphasis on
the front-end processing stage and the segmenter, and how these two stages provide
temporal abstraction.
Chapter 6 reports results of using the learning system on data segments obtained from
six patients during cardiac bypass surgery.
Chapter 7 discusses validity of the models learned, analyzes sources of error, and discusses
applicability of the system in diagnostic patient monitoring. Model variation across
time and across different levels of temporal abstraction and fault tolerance is also
examined.
Chapter 8 provides a summary of the main points from the thesis, and discusses promising
directions for future work.
16
Chapter 2
Qualitative Reasoning
In studying the behavior of dynamic systems, we often model the system with a set of
differential equations.
The differential equations capture the structure of the system by
specifying the relationships that exist among the functions of the system. From the differ-
ential equations and an initial state, we can derive a quantitative system behavior using
analytical methods or numerical simulation.
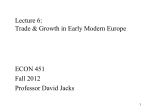
A qualitative abstraction of the above procedure allows us to work with an incomplete
specification of the system. A qualitative model can be represented by a set of qualitative differential equations, or qualitative constraints. From the constraints and an initial
state, we can derive a qualitative system behavior using qualitative simulation. Figure 2-1
!illustratesthis abstraction.
Different qualitative representations for models and their behavior have resulted from research in different problem domains [7]. In this chapter, we describe Kuipers' representation
in [20], used in his qualitative simulation system QSIM.
'2.1 Qualitative Model Constraints
QSIM represents a model of a system by a set of qualitative constraints applied to the
functions of the system. These include arithmetic constraints, which correspond to the basic
arithmetic and differential operators, and monotonic function constraints, which correspond
to monotonically increasing and decreasing functions that exist between two functions.
17
Perturbation
Dynamic System
System Behavior
Abstraction
Abstraction
Analytical Methods/Numerical Simulation
Quantitative
System Behavior
(Numerical Data)
Differential
Equations
Statistical Analysis (e.g. RegressionMethods)
Abstraction
Abstraction
Qualitative Simulation (e.g. QSIM)
Qualitative Constraints
(Qualitative Differential
Equations)
Qualitative
System Behavior
(Qualitative States)
Inductive Learning (e.g.GENMODEL)
Figure 2-1: Qualitative reasoning is an abstraction of mathematical reasoning with differential equations and continuously differentiable functions.
Arithmetic Constraints
Four arithmetic constraints are included in the QSIM representation:
1. add(f, g,h)
2. mult(f,g,h)
f(t) +g(t) = h(t)
f(t) x g(t) = h(t)
3. minus(f,g)
-f(t) =-g(t)
4. deriv(f, g) a
f'(t) = g(t)
Monotonic Function Constraints
When working with incomplete knowledge of a system, we may need to express a functional
relationship that exists between two system functions, without specifying the functional
relationship completely. In QSIM, the relationship can be described in terms of regions
that are monotonically increasing or decreasing, and landmark values that the functions
pass through. The QSIM representation includes two constraints for strictly monotonically
18
increasing and decreasing functional relationships. 1
f(t) = H(g(t)) where H(x) is a strictly monotonically increasing func-
1. M+(f, g) tion
2. M-(f,g)
=
f(t) = H(g(t)) where H(x) is a strictly monotonically decreasing
function
Note that since H(x) is a strictly monotonic function in both cases, both M+(f,g)
and M-(f,g)
require values of f(t)
and g(t) to have a one-to-one correspondence, i.e.
f(tl) = f(t 2 ) =- g(tl) = g(t2).
Also note that the two function constraints M + and M-
map onto many different
functions including exponential, logarithmic, linear and other monotonically increasing or
decreasing functions.
This many-to-one mapping enables qualitative models to capture
incomplete knowledge of a system.
Qualitative constraints can be considered as an abstraction of ordinary differential equations (ODE). Every suitable ODE can be decomposed into a corresponding set of qualitative
constraints. For example, Hooke's Law which relates the force of a spring to its displacement
with the Hooke's constant k [20]:
d2 x
dt 2
k
m
=--x
can be decomposed into the following qualitative constraints:
deriv(x, v)
v= d
a d
d2 x
-
dv
dt == deriv(v,a)
a = -- x == M-(a, x)
m
2.2
Qualitative System Behavior
A dynamic system is characterized by a number of system functions which vary over time.
The system behavior can be described in terms of these functions. In QSIM, system func1
In this thesis, M+ is also referred to as mplus and M- as mminus.
19
tions must be reasonablefunctions f: [a, b] -+ R* where * = [-oo, oo], which satisfy the
following criteria:
1. f is continuous on [a, b]
2. f is continuously differentiable on (a, b)
3. f has only finitely many critical points in any bounded interval
4. limt,a+f'(t) and limtb-f'(t)
exist in 2*. We define f'(a) and f'(b) to be equal to
these limits.
Every system function f(t) has associated with it a finite and totally ordered set of
landmark values. These include 0, the value of f(t) at each of its critical points, and the
value of f(t) at each of the endpoints of its domain.
The set of landmark values for a
function form its quantity space which includes all the values of interest for the function.
A value can be either at a landmark value, or in an interval between two landmark values.
The system has associated with it a finite and totally ordered set of distinguished time
points. These include all time points at which any of the system functions reaches a land-
mark value. The set of distinguished time points form a time space. A qualitative time
can be either a distinguished time point, or an interval between two adjacent distinguished
time points.
The qualitative state of f at t is defined as a pair < qval, qdir >. qval is the value of the
function at t, and is either a landmark value or an interval between two landmark values.
qdir is the direction of change of the function at t, and is one of inc, std, or dec depending
on whether the function is increasing, steady or decreasing at t.
Since f is a reasonable function, the qualitative state of f must be constant over intervals between adjacent distinguished time points. Therefore a function can be completely
characterized by its qualitative states at all its distinguished time points and at all intervals
between adjacent distinguished time points. Such a temporal sequence of qualitative states
of f forms the qualitative state history or qualitative behaviorof f.
Since a reasonable function f is continuously differentiable, the Intermediate Value
Theorem and the Mean Value Theorem restrict the possible transitions from one qualitative
state to the next. [20] includes a table listing all possible transitions.
20
2.3
Qualitative Simulation: QSIM
QSIM takes a qualitative model and an initial state, and generates all possible behaviors
from the initial state consistent with the qualitative constraints in the model. Starting
with the initial state, the QSIM algorithm works by repeatedly taking an active state and
generating all possible next-state transitions according to the table of possible transitions
mentioned in the previous section. These transitions are then filtered according to restrictions posed by the constraints in the system model. Because a model may allow multiple
behaviors, QSIM builds a tree of states representing all possible behaviors. Any path across
the tree from the given initial state to a final state is a possible behavior of the system.
2.4
Learning Qualitative Models: GENMODEL
GENMODEL [5]goes in the opposite direction to QSIM. It takes a system behavior and di-
mensional information about the system functions, and generates all qualitative constraints
that permits the system behavior. The GENMODEL algorithm works by first generating
all possible dimensionally correct qualitative constraints that may exist among the system
functions, according to different permutations of the functions. Then it progresses along
the state history, successivelypruning all constraints that are inconsistent with each state
transition. The set of qualitative constraints remaining at the end represent the most specific model that permits the given behavior.
Any subset of this model also permits the
given behavior, and therefore is also a possible model of the system.
2.5
An Example: The U-tube
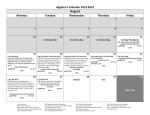
The QSIM representation can be illustrated by an example of a U-tube [20]. Figure 2-2
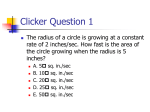
shows a U-tube (two partially filled tanks connected at the bottom by a tube).
If an increment of water is added to one arm (A) of the U-tube, the system will undergo
three different states before reaching equilibrium again:
Initial State The water level in A will rise to a new level with the water level in the other
arm (B) unchanged initially. There is a net pressure difference between the two arms,
resulting in a net flow of water from A to B.
21
A
B
I
I
I
I
(Normal)
t(O)
t(O)/t(l)
t(l)
Time, t
Figure 2-2: Qualitative states following addition of an increment of fluid to one arm of a
U-tube.
ITransitional State As time progresses, the level in A decreases and the level in B increases, while the pressure difference and the water flow diminishes.
Equilibrium State When the water in the two arms reach the same level, the pressure
difference and the water flow becomes zero and a new equilibrium is reached.
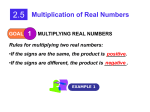
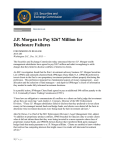
A simple model of the U-tube consists of six qualitative constraints, as illustrated in
Table 2-3 [6]:
1. The pressure in A increases with the level in A.
2. The pressure in B increases with the level in B.
3. The pressure difference between A and B is the difference in the two pressures in A
and B.
4. The flow from A to B increases with the pressure difference between A and B.
5. The level in A is inversely proportional to the derivative of the flow from A to B.
6. The level in B is proportional to the derivative of the flow from A to B.
These constraints are represented in a diagram in Figure 2-4.
2.5.1
Qualitative Simulation of the U-tube
With this simple model and a partial specification of the initial state, QSIM deduces the
remaining states according to the QSIM algorithm mentioned previously. The output of the
system behavior generated by running QSIM 2 on the U-tube model is shown in Figure 2-5.
2
We used an implementation
of QSIM in UNSW Prolog V4.2 on the HP9000/720 [6].
22
model(u_tube).
% function definitions
fn(a).
fn(b).
% level in arm a
% level in arm b
fn(pa).
fn(pb).
fn(pdiff).
fn(flow_ab).
% pressure in arm a
% pressure in arm b
% pressure difference
% flow rate from arm a to arm b
% model constraints
mplus(a,pa).
mplus(b,pb).
add(pb,pdiff,pa).
mplus(pdiff,flowab) .
inv_deriv(a,flow_ab).
deriv(b,flow_ab).
% initial conditions
of qualitative
state at t = t(O)
initialize(a,t(0),a(O)/inf,dec).
initialize (b,t () ,b(O),_).
% ordinal values for function landmarks
landmarks(a,[O,a(O),inf]).
landmarks(b,[O,b(O),inf]).
% definition of function values at normal equilibrium
normal( [a/a(O),
b/b(O),
pa/pa(O),
pb/pb(O),
pdiff/0,
flow_ab/O]).
:Figure 2-3: Prolog representation for the U-tube model, initialized for an increment of fluid
added to arm a.
23
_1
IT
Level A
·_
Pressure A
I\
I
I~
L1
Pressure Differenct
I
~zh
M+nA s
rluw
LauC.
-'
Figure 2-4: Qualitative model of a U-tube.
The qualitative states generated can be presented in qualitative plots as shown in Figure
2-6. In these plots, landmark values are placed on the vertical axis, and distinguished time
points and corresponding intervals are placed on the horizontal axis. The only positions
that can be taken at each time point are at or between landmark values.
2.5.2
Learning the U-tube Model
The system behavior described previously together with dimensional information on the system functions can be given to GENMODEL 3 to generate a set of all qualitative constraints
which are consistent with the behavior.
Dimensional information on the system functions of the U-tube are specified in Prolog
as follows:
units(a,mass).
units(b,mass).
units(pa,pressure).
units(pb, pressure).
units(pdiff,pressure).
units(flow_ab,mass/t).
The output of the U-tube model generated by GENMODEL on the given behavior
3
GENMODEL is implemented in UNSW Prolog V4.2 on the HP9000/720 [5].
24
Simulating u_tube
t(O)
t(O) / t(1)
t(1)
simulation completed
landmarks used in simulation:
landmarks(a,
landmarks(b,
[0, a(O), a(1),
[0, b(O), b(1),
inf]).
inf]).
landmarks(pa,
[0, pa(O), pa(1),
landmarks(pb,
[0, pb(O), pb(1),
landmarks(pdiff,
[0, inf]).
landmarks(flowab,
[0, inf]).
inf]).
inf]).
The simulation generated the following qualitative states:
t(0)
a
b
a(O) / inf
b(O)
dec
inc
pa
pb
pa(O) / inf
pb(O)
dec
inc
pdiff
0 / inf
dec
flowab
0 / inf
dec
a
b
a(O) / inf
b(O) / inf
dec
inc
pa
pa(O) / inf
dec
pb
pb(O) / inf
inc
pdiff
0 / inf
dec
flowab
0 / inf
dec
a
b
a(1)
b(1)
std
std
pa
pa(1)
std
pb
pdiff
flowab
pb(1)
0
0
std
std
std
t(O) / t(1)
t(1)
Figure 2-5: Output of the system behavior generated by running QSIM on the U-tube
model.
25
lnf
I-lA(A)
inf
:(I)
vrl(B)
b(I)
b(O)
a(O
t(0)
t(0)
t(1)
-'n
t(1)
-inf
inf.
prss..r(A)
inf
preun.(B)
pb(l)'
pb(O)
1
p( )
P(O
t(O)
t(l)
(t()
-inf
'
t()
-inf
I
t(o)
l
t (A-B)
prrressru
diffnce
inf
t(1)
-inf
I
I
Figure 2-6: Qualitative plots for the qualitative states of a U-tube following addition of an
increment of fluid to one arm until equilibrium is reached.
is shown in Figure 2-7. In the case of the U-tube, the generated model is equivalent to
the original model after redundancy elimination by GENMODEL. GENMODEL will be
described further in Chapter 3.
26
Generating possible constraints
mplus(pdiff, flowab)
mplus(pdiff, a)
mplus(pdiff, pa)
mplus(flowab, pdiff)
mplus(flow-ab, a)
mplus(flow-ab, pa)
mplus(a, pdiff)
invderiv(a, flow-ab)
mplus(a, flow_ab)
mplus(a, pa)
deriv(b, flowab)
mplus(b, pb)
mplus(pa, pdiff)
mplus(pa, flowab)
mplus(pa, a)
mplus(pb, b)
add(pdiff, pb, pa)
add(pa, pb, pdiff)
add(pb, pdiff, pa)
add(pb, pa, pdiff)
filtering with state t(O) / t(1)
filtering with state t(1)
filtering : mplLus(pdiff, a)
filtering : mp].us(pdiff, pa)
filtering : mpllus(flowab, a)
filtering : mp].us(flow_ab,pa)
filtering : mp]lus(a, pdiff)
filtering : mpl.us(a, flowab)
filtering : mp]lus(pa, pdiff)
filtering : mpllus(pa, flow-ab)
filtering : addL(pa, pb, pdiff)
filtering : addL(pb, pa, pdiff)
Checking for redundancies
filtering : mpllus(flowab, pdiff) simple redundancy
filtering : mp].us(pa, a) simple redundancy
filtering : mpllus(pb, b) simple redundancy
filtering: add((pb, pdiff, pa) simple redundancy
Model Constraints:
deriv(b, flow-ab)
invderiv (a, flow-ab)
mplus(pdiff, flowab)
mplus(a, pa)
mplus(b, pb)
add(pdiff, pb, pa)
Figure 2-7: Output of the U-tube model generated by GENMODEL on the given behavior.
Note that the model learned is the same as the original model shown previously.
27
Chapter 3
Learning Qualitative Models
In this chapter, we examine the learnability of qualitative models employing the QSIM
formalism [20]. We review the Probably Approximately Correct (PAC) model of learning
[37], and show that QSIM models are efficiently PAC learnable from positive examples only.
The proof is based on the algorithm GENMODEL [5]which can efficiently construct a QSIM
model consistent with a given set of examples, if one exists. The chapter continues with
a detailed coverage of GENMODEL, including the newly added features of dimensional
analysis and fault tolerance, and a comparison of GENMODEL with other approaches of
learning qualitative models. We end the chapter with a discussion of the difficulties of
applying PAC results to our task of learning QSIM models from physiological signals.
3.1 Probably Approximately Correct Learning
A common setting in machine learning is as follows: Given a set of examples, produce a
concept consistent with the examples that is likely to correctly classify future instances. We
are interested in algorithms that can perform this task efficiently. The Probably Approximately Correct (PAC) model of learning introduced by Valiant [37] is an attempt to make
precise the notion of "learnable from examples" in such a setting [17, 30].
3.1.1
Definitions
Let X be the set of encodings of all instances.
X is called the instance space. In our
learning task, X is the set of all qualitative states within a given set of landmark values
and distinguished time points.
28
A concept c is a subset of the instance space, i.e. c C X. In our learning task, c is a QSIM
model which can be seen as a concept specifying a subset of X (the set of all qualitative
states) as legal states. We can equivalently define a concept c to be a boolean mapping
applied to X, i.e. c : X-+ (0, 1}. An example is considered to be a positive example if
c(x) = 1, and a negative example if c(x) = 0.
A concept class C over X is a collection of concepts over X. In our case, C is the set
of all QSIM models with a given number of system functions. The goal of the learning
algorithm is to determine which concept in C (the target concept c) is actually being used
in classifying the examples seen so far.
We define n to be the size parameter of our instance space X. In our case, n is the
number of system functions in our system. Note that n affects the number of possible
qualitative states and thus the size of the instance space X. The difficulty of learning a
concept that has been selected from Cn depends on the size ICn I of Cn. Let 1
An= lg Cl
An may be viewed as the minimum number of bits needed to specify an arbitrary element
of Cn. If An is polynomial in n, Cn is said to be polynomial-sized. We are interested in
characterizing when a class C of concepts is easily learnable from examples.
3.1.2
PAC Learnability
Stated informally, PAC learnability is the notion that the concept acquired by the learner
should closely approximate the concept being taught, in the sense that the acquired concept
should perform well on new data drawn according to the same probability distribution as
that according to which the examples used for learning are drawn.
We define Pn as the probability distribution defined on the instance space Xn according
to which the examples for learning are drawn. The performance of the acquired concept c' is
measured by the probability that a new example drawn according to Pn will be incorrectly
classified by c'. For any hypothesized concept c' and a target concept c, the error rate of c'
is defined as:
error(c')= Prepn[c'(x) $ c(x)]
llg x = log2 x
29
where the subscript x E P, indicates that x is drawn randomly according to P,.
We would like our learning algorithm A to be able to produce a concept whose error rate
is less than a given accuracy parameter
with 0 < e < 1. However, we cannot expect this
to happen always, since the algorithm may suffer from "bad luck" in drawing a reasonably
representative set of examples from Pn for learning.
Thus we also include a confidence
parameter 6 with 0 < 6 < 1 and require that the probability that A produces an accurate
answer be at least 1 - 6. As
and
approach zero, we expect A to require more examples
and computation time.
We would like the learning algorithm to satisfy the following properties:
* The number of examples needed is small.
* The amount of computation performed is small.
* The concept produced is accurate, i.e. the error rate
is arbitrarily small.
* The algorithm produces such an accurate concept most of the time, i.e. with a probability of 1 - 6 that is arbitrarily close to 1.
The concept class C is said to be efficiently PAC learnable if there exists an algorithm A
for learning any concept c E C that satisfies the above criteria.
To define PAC learnability formally, we say that a concept class C is efficiently PAC
learnable if there exists an algorithm A and a polynomial s(.,.,
6, all probability distributions P, on X,
) such that for all n, , and
and all concepts c E Cn, A will with probability
at least 1 - 6, when given a set of examples of size m = s(n, l, ~) drawn according to P,
output a c' E Cn such that error(c') < e. Furthermore, A's running time is polynomially
bounded in n and m.
The hypothesis c' E C of the learning algorithm is thus approximately correct with high
probability, hence the acronym PAC for Probably Approximately Correct.
3.1.3
Proving PAC Learnability
One approach of PAC learning due to Blumer et al. [3] is as follows: Draw a large enough
set of examples according to P, and find an algorithm which, given the set of examples,
outputs any concept c E Cn consistent with all the examples in polynomial time. If there
exists such an algorithm for the concept class C, C is said to be polynomial-time identifiable.
30
Formally, we say that C is polynomial-time identifiable if there exists an algorithm A and
a polynomial p(A, m) which, when given the integer n and a sample S of size m, produces
in time p(A,, m) a concept c E C consistent with S, if such a concept exists.
This leads to an interesting interpretation of learning. Learning can be seen as the act
of finding a pattern in the given examples that allows compression of the examples. We can
measure simplicity by the size of the concept space of the algorithm, or equivalently by An,
the minimum number of bits needed to specify a concept c among all the concepts in C,.
An algorithm that finds a succinct hypothesis consistent with the given examples is called
an Occam algorithm. This formalizes a principle known as Occam's Razor which equates
learning with the discovery of a "simple" explanation for the observed examples. A concept
that is considerably shorter than the examples is likely to be a good predictor for future
data [29].
Next we look at how large a set of examples is "large enough" for PAC learning.
[3]
includes a key theorem on this issue.
Theorem
Given a concept c E Cn and a set of examples S of c of size m drawn according
to P, the probability is at most
ICnl (1- e)m
that there exists a hypothesis c' E C, such that:
* the error of c' is greater than , and
· c' is consistent with S.
Proof
If c' is a single hypothesis in C, of error greater than
, the chance that c' is
consistent with a randomly drawn set of examples S of size m is less than (1 -
)m .
Since C, has ICnI members, the chance that there exists any member of C, satisfying
both conditions above is at most
-
ICE(1
E)m . ·
Using the inequality
-x
< e- x
we can prove that
1
m >- (ln Cnl+In
E
31
1
implies that
ICnl(l- E)m <
Thus if m satisfies the above lower bound, the probability is less than 6 that a hypothesis
in Cn which is consistent with S will turn out to have error greater than e. Therefore to
PAC learn a concept, the learning algorithm need only examine m examples where m has
a lower-bound as follows: 2
m=
Q(-(In lCn + n))
Recall if Cn is polynomial-sized, then An and therefore In ICn is polynomial in n. Therefore
m is polynomial in n,
and
To conclude, an algorithm that draws m examples according to Pn and outputs any
concept consistent with all the examples in polynomial time is a PAC learning algorithm.
Thus if Cn is polynomial-sized and polynomial-time identifiable, then it is efficiently PAC
learnable.
3.1.4
An Occam Algorithm for Learning Conjunctions
In [37] Valiant provides an algorithm for PAC learning the set of boolean formulae in
conjunctive normal form (CNF) where each clause contains at most k literals. This set of
boolean formulae is known as k- CNF. The algorithm is capable of PAC learning from positive
examples only. In Section 3.3.2 we will map the problem of identifying a QSIM model
consistent with a given set of examples to the problem of identifying a k-CNF consistent
with a given set of examples.
First we calculate the number of examples needed. The number of conjunctions over
the boolean variables x1,..., Xn is 3n since each variable either appears as a positive or
negative literal, or is absent entirely. Applying the formula for the lower bound in the
previous section, we see that a sample of size O(n + in
is sufficient to guarantee that
the hypothesis output by our learning algorithm is e accurate with confidence of at least
1 -J.
The algorithm starts with the hypothesis conjunction which contains all the literals:
c' = X1A
1
A..
2A = Q(B) denotes B is a lower bound of A.
32
A
An
Upon each positive example x, the algorithm updates c' by deleting the literal xi if xi = 0
in the example, and deleting the literal xi if xi = 1 in the example. Thus the algorithm
deletes any literal that contradicts the data. This can be seen as starting with the most
specific concept and successively generalizing the concept upon each positive example given.
Since the algorithm takes linear time to process each example, given m examples with
m as calculated above, the running time is bounded by mn and hence is bounded by a
polynomial in n,
1
and . Therefore this is an efficient PAC learning algorithm for the class
of k-CNF.
3.2
The GENMODEL Algorithm
GENMODEL is a program for generating qualitative models from example behaviors [5].
Given a set of qualitative states describing a system behavior, GENMODEL outputs all
QSIM constraints consistent with the state history. Together, these constraints form the
most specific QSIM model given the example behavior.
The Algorithm
Input:
* A set of system functions, Functions.
* A set of units for the system functions, Units
* A set of landmark lists for the system functions, Landmarks.
* A set of qualitative states, States.
Output:
A qualitative model which consists of all constraints that are consistent with the state
history and dimensionally correct, Model.
Functions used:
search() A function for searching corresponding values from a set of qualitative states.
dimcheck()
A function for checking dimensional compatibility of functions within a
constraint.
33
begin
Constraints+-0;
Correspondings - search(States);
for each f, f2 in Functions such that fl
# f2 do
for each predicate2 in {inv, deriv, invderiv, M +, M-} do
fl, f2, Units) then
if dimcheck(predicate2,
add predicate2(fl,f 2) to Constraints;
for each f,
f2,
f3 in Functions such that f # f2#f3 do
for each predicate3 in {add, mult} do
fl, f2, f3, Units) then
if dimcheck(predicate3,
add predicate3(fl,f2,f3) to Constraints;
for each s in States do
for each c in Constraints do
if not check(c, s, Landmarks, Correspondings) then
delete c from Constraints;
reduce(Constraints);
Model+- Constraints;
end
Figure 3-1: GENMODEL algorithm.
check() A function for checking validity of a constraint given a qualitative state and
sets of corresponding values.
reduce() A function for removing redundancy from constraints.
For example, since
M+(A, B) and M+(B, A) specify the same relationship, one of them can be
removed.
Method:
* Search the entire state history States for sets of corresponding values.
* Generate the initial search space by constructing all dimensionally correct constraints with different permutations of system functions in Functions.
* Successivelyprune inconsistent constraints upon each qualitative state in States.
* Remove redundancy from the remaining constraints
* Output the result as a qualitative model.
The entire algorithm is shown in Figure 3-1.
34
3.3
QSIM Models are PAC Learnable
From Section 3.1.3 we conclude that to prove that the concept class of QSIM models is PAC
learnable, it suffices to prove that the class is polynomial-sized and that it is polynomial-time
identifiable. The following two sections provide these proofs.
3.3.1
The Class of QSIM Models is Polynomial-Sized
To show that the concept class of QSIM models is polynomial-sized, we begin by noting
that in the QSIM formalism there are five kinds of two-function constraints (inv, deriv,
invderiv,
M+ and M-), and two kinds of three-function constraints (add and mult).
Therefore with n system functions, the number of possible QSIM constraints N is as follows:
N = 5n(n - 1) + 2n(n - 1)(n- 2)
Therefore, the number of possible QSIM models is:
IQSIM-Models(n)l= 2N = 25n(n-1 )+2n(n-1)(n-2)
since each QSIM constraint can either be present or absent in the model. This implies that:
lg (QSIM-Models(n)I) = N = O(n3 )
Therefore the concept class of QSIM models is polynomial-sized.
To PAC learn a QSIM model, we need m examples where m is calculated as follows:
m=Q
3.3.2
((5n(n - 1) + 2n(n - 1)(n - 2))ln2 + In ))
QSIM Models are Polynomial-Time Identifiable
In this section we show that GENMODEL is an algorithm for efficiently constructing a
QSIM model consistent with a given set of examples.
We prove this by mapping the
problem of identifying a QSIM model consistent with a given set of examples to the problem
of identifying a k-CNF consistent with a given set of examples. The algorithm presented
in Section 3.1.4 then yields an algorithm for identifying a QSIM model consistent with a
35
given set of examples in polynomial time. We show that this algorithm is in fact identical
to GENMODEL.
We view each QSIM model as a conjunction of QSIM constraints, and each QSIM
constraint as a boolean variable.
Then learning QSIM models is equivalent to learning
monotone conjunctions 3 with N boolean variables, where N is the number of possible
QSIM constraints as calculated in the previous section.
Now the algorithm starts with the hypothesis of a monotone conjunction which contains
all N of the boolean variables, i.e. all possible QSIM constraints:
C'=xlA
Ax,n
The qualitative states provided for learning constitute the positive examples.
Upon
each positive example x, the algorithm updates c' by deleting the boolean variable xi if
the corresponding QSIM constraint is inconsistent with the example. Since each boolean
variable xi corresponds to a QSIM constraint, the algorithm prunes any constraint that is
inconsistent with each qualitative state. This can be seen as starting with the most specific
model and successively generalizing the model upon each qualitative state given. This is
identical to the approach taken by GENMODEL.
Now it remains to show that GENMODEL takes polynomial time to process each qualitative state. We review each step taken by GENMODEL in learning a QSIM model:
* Search the entire state history for sets of corresponding values. For m qualitative
states, there are at most m sets of corresponding values, and the search takes O(m)
time.
* Generate the initial search space by constructing all constraints with different permutations of system functions. For n system functions, this takes O(n3 ) time as shown
in the previous section.
* Successivelyprune inconsistent constraints upon each qualitative state. Checking for
consistency of a constraint with a qualitative state involves:
- Checking landmark values and directions of change. This takes linear time.
3
Monotone conjunctions are ones with positive literals only.
36
- Checking corresponding values. Since there are at most m sets of corresponding
values, this takes O(m) time.
* Remove redundancy from the remaining constraints. Since we started off with O(n3 )
constraints, there are at most the same number of constraints remaining in the final
model. Therefore, removing redundancy takes O(n3 ) time.
* Output the result as a qualitative model.
Therefore for GENMODEL the processing time of each qualitative state is polynomial in
m and n.
Since the algorithm takes polynomial time to process each qualitative state, given m
states with m as calculated above, the running time is bounded by p(m, n) where p(-, ) is a
polynomial in the two arguments. Therefore the running time is bounded by a polynomial
in n,
and <. Therefore this is an efficient PAC learning algorithm for the concept class of
QSIM models.
3.4
GENMODEL
In this thesis, the original implementation of the GENMODEL program described in [5] is
extended to include dimensional analysis and fault tolerance.
3.4.1
Dimensional Analysis
Dimensional analysis is an effective way of significantly reducing the size of the initial
search space of constraints. Before generating a constraint, GENMODEL checks for units
compatibility among functions within the constraint. This is similar to the approach used in
several other inductive learning systems, including ABACUS [8], a system for quantitative
discovery, and MISQ [28], a system based upon GENMODEL.
The dimension of each function is specified at the beginning, usually in terms of the
type of quantity the function represents, e.g. 1/time for the heart rate (HR), volume for
the stroke volume (SV), and volume/time for the cardiac output (CO). This allows the
constraint mult(HR, SV, CO) to be generated since (1/time) x (volume) = volume/time,
but does not allow mult(HR, CO, SV) or add(HR, SV, CO) to be generated since they are
37
dimensionally incorrect. Note that the functional constraints M + and M- are not restricted
by dimensions.
3.4.2
Performance on Learning the U-Tube Model
With dimensional analysis, GENMODEL comes up with exactly the six constraints for the
U-tube system described in Section 2.5, given the three qualitative states describing the
example behavior. 4 This is a significant improvement to previous results reported in [5] in
which 14 constraints were obtained.
3.4.3
Version Space
In [24], Mitchell points out that generality forms a partial order among elements in the
concept space. This partial order allows the set H of plausible hypotheses at each stage
of learning to be represented by its most generalelements (upper bounds) G, and its most
specific elements (lower bounds) S, as illustrated in Figure 3-2. A plausible hypothesis is
defined as any hypothesis that has not yet been ruled out by the examples seen so far. The
set H of all plausible hypotheses is called the version space.
Mitchellproposes a learning algorithm, calledthe candidate-eliminationalgorithm,based
on this boundary-set representation of H. Initially, the version space contains all possible
concepts. As training examples are presented to the learning program, inconsistent concepts
are eliminated from the space until only one concept remains - the target concept.
Each positive example causes the program to generalize elements in S as little as possible,
so that they will cover the example. This is called the Update-S routine. Conversely, each
negative example causes the program to specialize elements in G as little as possible, so that
they will not cover the example. This is called the Update-G routine. The version space
gradually shrinks in this manner until only the target concept remains.
In the task of learning QSIM models, the most specific concept at each stage is unique.
It is the model which consists of all the QSIM constraints consistent with all the qualitative
states presented so far. Since GENMODEL successively updates the most specific model
by pruning constraints that are inconsistent with the most current example, it is equivalent
to the Update-S routine in Mitchell's Candidate-elimination
4
Learning Algorithm.
The U-tube system is a standard reference problem in the qualitative modeling community.
38
more
general
O ......
--
A model consisting of no
constraints (the null description)
- the most general concept
G
S
A model consisting of all
possible constraints
-
e
InostCaLe
morespecific
LUILtfL
H - the set of all plausible hypotheses (the version space)
G - the set of most general plausible hypotheses (the upper boundary set)
S - the set of most specific plausible hypotheses (the lower boundary set)
Figure 3-2: Using the upper and lower boundary sets to represent the version space.
3.4.4
Fault Tolerance
For domains involving noisy learning data, such as noisy signals from hemodynamic monitoring, it is difficult to implement front-end signal processing which filters the noise and
restores the signals completely. Part of the difficulty lies in the nature of the noise. Hemodynamic monitoring is vulnerable to a wide variety of artifacts.
These include artifacts
resulting from various kinds of clinical interventions which we will describe in Section 5.2.1.
These artifacts are relatively easy to detect because their values are usually outside the
physiologically attainable range. There are also artifacts which do not affect the signals
so drastically, and therefore can be hard to detect. For example, patient movements can
sometimes affect the operation of transducers and alter the shape of the signals obtained,
thereby affecting the qualitative state history subsequently generated. It is hard if not
impossible to restore the original signal from a signal heavily distorted by artifacts.
To
accommodate such difficulties in obtaining a perfectly clean signal for segmentation, we
need to incorporate a degree of fault tolerance into GENMODEL.
A simple approach is to tag a counter onto every constraint in the initial search space.
39
begin
Constraints+- 0;
Correspondings+- search(States);
for each fl, f2 in Functions
such that f
4 f2 do
M,+ , M-} do
for each predicate2 in {inv, deriv, inv_deriv, M
if dimcheck(predicate2,
fl, f2, Units) then
add < predicate2(fl, f2), 0 > to Constraints;
for each fl, f2, f3 in Functions such that fl 0 f2#f3 do
for each predicate3 in {add, mult} do
if dimcheck(predicate3, fl, f2, f3, Units) then
add < predicate3(fl, f2, f3), 0 > to Constraints;
for each s in States do
begin
Remaining e 0
for each < c, i > in Constraints do
if check(c, s, Landmarks, Correspondings) then
add < c, i > to Remaining
else
if (i < TOLERANCE) then
add < c, (i + 1) > to Remaining
Constraints+- Remaining
end
reduce(Constraints);
Model --Constraints;
end
Figure 3-3: GENMODEL algorithm with fault tolerance.
'This counter keeps track of how many states the constraint has failed in so far. We set a noise
level
to a fraction of the total number of states in the example behavior. A constraint has
to be inconsistent with this many states before it is pruned. The GENMODEL algorithm
modified to include fault tolerance is shown in Figure 3-3.
3.4.5
Comparison of GENMODEL with Other Learning Approaches
GENMODEL does not require negative examples.
The greatest strength of GENMODEL is that it learns from positive examples only. There
is no need to generate negative examples as needed in other inductive learning approaches
such as GOLEM and genetic algorithms.
In [4], Bratko et al. report that learning the U-tube model with GOLEM requires six
40
hand-generated negative example states, in addition to the same positive example behavior
we used for GENMODEL which consists of only three states.
On each iteration in the
GOLEM algorithm, a fixed number of clauses are first generated by Relative Least General
Generalization (RLGG) [27]. The clause that covers the most positive examples and none
of the negative examples is then chosen for propagation to the next iteration.
In [38], Var§ek's genetic algorithm approach requires 17 positive example states and 78
negative example states to learn the U-tube model. In each cycle, candidate solutions are
selected for "reproduction" based on a fitness function which is the sum of the fraction of
positive and negative examples covered correctly and a "bonus" indicating the size of the
solution.
In both approaches, it is therefore essential for the user to give the "right" negative
examples. Badly chosen negative examples or an inadequate number of them will cause
an inappropriate clause to be propagated to the next iteration, which will ultimately affect
the concept output in the end. However, there are no existing rules to guide the selection
of negative examples.
A trial-and-error approach can be tedious, especially in complex
domains such as human physiology.
GENMODEL does not require ground facts for background knowledge
In GENMODEL, the definitions of the QSIM representation are inherent in the check()
function used for checking consistency of a constraint with a given qualitative state. There
is no need to generate explicit ground facts 5 for this background knowledge, as needed in
GOLEM.
GOLEM accepts definitions of background predicates in terms of ground facts.
In
learning QSIM models, explicit ground facts describing QSIM constraint definitions must
be generated according to functions and landmark lists relevant to the modeling problem
at hand. In [4], Bratko et al. report that learning the U-tube model requires a total of 5408
ground facts as background knowledge. This is already a simplification which excludes rules
regarding corresponding values in the M + and M- constraints, rules regarding consistency
of infinite values in the add constraint, and rules on the mult constraint. In a more complex
domain such as human physiology which potentially involves long landmark lists, the size
of the background knowledge required can grow exceedingly large.
5
A clause is said to be ground if it does not contain any variables.
41
GENMODEL is guaranteed to produce a correct model if one exists.
Given a set of qualitative states representing a system behavior, GENMODEL successively
prunes inconsistent constraints upon each state. The constraints remaining in the end forms
the output model. Therefore, GENMODEL is guaranteed to produce a correct model if one
exists.
On the other hand, GOLEMand genetic algorithms perform heuristic searches across the
concept space. GOLEM performs hill climbing with positive and negative example coverage
as the heuristic guiding the search. Genetic algorithms similarly perform hill climbing with
the fitness function serving as the heuristic. Since neither heuristic is a perfect quality
measurement of the current model, GOLEM and genetic algorithms are not guaranteed to
produce a correct model even if one exists, unless the search becomes exhaustive.
3.5
Applicability of PAC Learning
As discussed in Section 3.3, the following is a PAC learning algorithm for learning a QSIM
model from physiological signals:
1. Obtain m qualitative states where m is calculated as follows:
m=
1
n
1
((ln2N + n )) = Q( ((5n(n- 1)+ 2n(n- l)(n - 2))ln2 + n ))
2. Learn a QSIM model from the m qualitative states using GENMODEL.
Applying this algorithm to our learning task is difficult for the following reasons:
* Qualitative states cannot be modeled as independent examples drawn from an underly-
ing probability distribution. Given a reasonable function and a qualitative state, there
are only a limited number of possible transitions the system can make, as described in
[20]. Further, successive states in signals obtained from hemodynamic monitoring are
highly correlated because of physiological constraints limiting for instance the rate of
change of signals.
* For our experiments, we use 8 different signals. Therefore n = 8. To PAC learn a
QSIM model with an accuracy and a confidence level of 80%, i.e.
= 6 = 0.2, we need
m = 3308 qualitative states. From our experience in segmentation, this translates to
42
about 80-90 hours of patient data. Even to do so with an accuracy and a confidence
level of just 50%, i.e.
=
= 0.5, we still need m = 1322 qualitative states. This
translates to about 30-40 hours of patient data. In such a long time span, the patient
condition and therefore the corresponding model may have already changed.
Signals from hemodynamic monitoring are corrupted by various artifacts and noise.
The PAC learning algorithm previously developed assumes learning examples to be
noise-free.
Therefore, for our learning task, we will apply GENMODEL for polynomial-time identification of a QSIM model from qualitative states only. We will not observe the sample
complexity for PAC learning. Even so, as we will see in Chapter 6, we still obtain useful
models of reasonable size.
43
Chapter 4
Physiological Signals and Models
4.1
Hemodynamic Monitoring
Hemodynamic monitoring provides information on the performance of the cardiovascular
(CV) system, and allows the physician to manipulate the CV system with fluids and drugs
in the critically ill patient or during surgical procedures.
Real time hemodynamic mea-
surements cover many aspects of the CV system, including heart rate, blood pressures,
temperatures, oxygen supply and others. In this thesis, we use eight signals derived from
such measurements for learning a qualitative model that describes the CV system. The
basic CV parameters and their characteristics will be reviewed in the following section.
4.1.1
Primary Measurements
Heart Rate (HR)
The heart rate is determined from the electrocardiogram (ECG) signal as the reciprocal of
the interval between two successive QRS complexes. (QRS complexes are the large voltage
spikes that correspond to ventricular contraction.) In our experiments, the heart rate signal
is sampled at 1 Hz.
Arterial Blood Pressure Waveform (ABP)
The arterial blood pressure waveform in our data comes from invasive monitoring by a
catheter. Invasive monitoring enables recording of rapidly changing arterial pressures, as
opposed to noninvasive methods such as the auscultatory detection of Korotkoff sounds.
44
ABP,
Systolic pressure
(- 120 mmHg)
Mean pressure
(- 96 mmHg)
Diastolic pressure
(- 80 mmHg)
.
0
0.5
1.0
Time/s
Figure 4-1: Deriving the systolic, diastolic and mean pressures from the arterial blood
pressure waveform.
The signal in our data is sampled at 125 Hz.
From the ABP waveform, the following signals can be determined (Figure 4-1):
Systolic arterial blood pressure (ABPS) - the value at the height of an ABP pulse.
Diastolic arterial blood pressure (ABPD) - the value at the lowest point of an ABP
pulse.
Mean arterial blood pressure (ABPM) - the mean value of an ABP pulse. This can
be calculated by dividing the area under the pulse by the duration of the pulse:
ABPM = ABPdt
b-a
where a is the starting time of the pulse and b is the ending time of the pulse [11].
These signals are derived at 1 Hz.
Central Venous Pressure (CVP)
Blood from all the systemic veins flows into the right atrium. Therefore, the pressure in
the right atrium is called the central venous pressure.
Cardiac output curves (from the
Frank-Starling law of the heart) can be obtained by plotting the cardiac output versus the
CVP [11].
45
The central venous pressure in our data comes from invasive monitoring by a catheter.
The waveform is sampled at 125 Hz. The mean CVP signal (CVPM) at 1 Hz is used in our
experiments.
Temperature
(Tskin, Tcore)
The skin temperature and the core temperature are recorded at 1 Hz. From these two
signals, a skin-to-core temperature gradient can be determined as described in Section 4.1.2.
4.1.2
Derived Values
From the primary measurements, various useful indices of cardiovascular function may be
calculated
as follows [25, 31].
Stroke Volume (SV)
During diastole, the ventricles are filled to about 120-130 ml. This volume is known as the
end-diastolic volume. During systole, the ventricles are emptied to a remaining volume of
about 50 to 60 ml. This volume is known as the end-systolic volume. The difference between
the end-diastolic volume and the end-systolic volume is the volume of blood pumped out of
the ventricles during systole. This volume is about 70 ml, and is called the stroke volume
[11].
The pulse contour method developed by Wesseling et al. for deriving the stroke volume
(SV) and cardiac output (CO) from the arterial pressure waveform has been studied widely
in the research literature [40, 15, 34, 10, 36, 39]. Unlike methods such as the thermodilution
technique which allows for only intermittent measurements of CO, the pulse contour method
enables continuous monitoring of CO, which is important for the management of critically
ill patients whose clinical conditions may change rapidly.
The pulse contour method estimates the stroke volume from the arterial blood pressure
waveform as the systolic ejection area Asys (Figure 4-2) divided by a constant Zao representing the characteristic impedance of the aorta. 1 The systolic ejection area is represented
by the integral of the difference between the arterial blood pressure waveform (ABP) and
1The pulse contour method is based on the "Windkessel" model of the systemic circulation which relates
the arterial pressure difference to the blood flow via the impedance through which the flow is driven. The
stroke volume can be calculated from the pressure as the driving force for flow during the ejection time.
46
ABP/mmHg
nichrnfir nntrh
...
systolic pressure
I
100
nintrairnrocllo
---
Systolic
Ejection
Period
I
Aortic valve
opens
An
0
0.5
1.0
Time/s
Figure 4-2: Deriving the stroke volume from the arterial blood pressure waveform.
the diastolic arterial blood pressure (ABPD) over the systolic ejection period (SEP) 2:
SV = Asys_ ftESEp(ABP- ABPD) dt
Zao
Zao
Zao
has been shown to be relatively constant over short periods. Since the segments used
in our experiments are 16.7 minutes long, the relatively constant Zao does not affect the
qualitative behavior of the function and can be disregarded.
The results obtained by the pulse contour method and standard techniques such as
thermodilution have been shown to correlate well even under dynamic conditions such as in
patients undergoing coronary artery bypass surgery [15, 10], patients in surgical intensive
care units [36], patients undergoing manipulations of blood pressure [39], and patients
undergoing treatments involving vasoactive drugs [34].
2
The end of the systolic ejection period is marked by the dichrotic notch formed at the closure of the
aortic valve.
47
Cardiac Output (CO)
The cardiac output is the rate of blood flow from the left ventricle into the aorta. It is
related to the heart rate and the stroke volume by the followingequation:
CO= HR x SV
Ventricular Contractility (VC)
VC = d(ABP)
dt
peak
Experimental studies have shown that the rate of rise of arterial blood pressure in general
correlates well with the strength of contraction of the ventricle. The peak
d(ABP)
which
occurs at the onset of systole, is often used as an indicator of ventricular contractility
[11, 25, 31].
Skin-to-core Temperature Gradient (AT)
AT = Tcore- Tskin
The difference between the skin and core temperatures of the body is a good indicator of
the degree of vasoconstriction,
i.e. the state of contraction of the vascular tree. A rise
in this differential indicates increasing vasoconstriction while a fall indicates vasodilation.
The degree of vasoconstriction in turn reflects cardiac output.
Under conditions of poor
cardiac output, as in hypovolemia,the body responds by trying to raise the blood pressure
by vasoconstriction, at the expense of tissue perfusion [25, 42].
Rate Pressure Product (RPP)
RPP = HR x ABPS
The rate pressure product (RPP) is the product of the heart rate (HR) and the systolic
arterial blood pressure (ABPS). Studies in animals [41] and humans [9] have shown that
48
the RPP correlates well with the myocardial oxygen consumption (mVO 2 ), which is closely
related to the work of the heart. mVO 2 depends on several factors, including heart rate,
ventricular contractility and ventricular wall tension. RPP is an easy variable to derive,
and is clinically useful as an indicator for the appropriate limit of safe ventricular work.
4.2
A Qualitative Cardiovascular Model
In this section, we describe a set of possible qualitative constraints that may exist among
the different variables of hemodynamic monitoring described in the previous section. These
constraints form a "gold-standard"
target model of the CV system which allows us to
compare our experimental results and evaluate the performance of the learning system.
Because of the enormous complexity of the CV system, formulating a model is by no
means a simple task. The constraints included in this section are not meant to be a comprehensive coverage of the CV system. For a more detailed coverage, textbooks on medical
physiology such as [11] can be consulted.
Furthermore, different models may exist for
different clinical conditions; a constraint may be valid only under certain conditions.
Relationship Among Heart Rate, Stroke Volume and Cardiac Output
The heart rate (HR), stroke volume (SV) and cardiac output (CO) are related by the
following equation:
CO = HR x SV
This translates into the followingqualitative constraint:
mult(HR, SV, CO)
Relationship Among Heart Rate, Arterial Blood Pressure and Rate Pressure
Product
The heart rate (HR), systolic arterial blood pressure (ABPS) and rate pressure product
(RPP) are related by the following equation:
RPP = HR x ABPS
49
Cardiac Output (CO)
is
5
0
-4
0
+4
+
+12
Central VenousPressure(CVP) / mmHg
Figure 4-3: Cardiac output curves for the normal heart and for hypo- and hypereffective
hearts.
Since the behavior of the mean arterial blood pressure (ABPM) approximates that of the
systolic arterial blood pressure (ABPS) well in most circumstances, the following qualitative
constraint is valid in general:
mult(HR, ABPM, RPP)
The Frank-StarlingLaw of the Heart
The Frank-Starling law states that within physiological limits, the heart pumps all the
blood that comes to it without allowing excessivedamming of blood in the veins. In other
words, the greater the heart is filled during diastole, the greater will be the quantity of blood
pumped into the aorta. The heart automatically adapts itself to the amount of blood that
flows into it from the veins, as long as the total quantity does not exceed the physiological
limit that the heart can pump.
Cardiac output curves (Figure 4-3) illustrate the Frank-Starling law [11]. They show
the relationship between the central venous pressure (CVP) (i.e. the right atrial pressure)
at the input of the heart and cardiac output (CO) from the left ventricle in different conditions. From the curves, we see that CO increases with CVP until when the venous return
overwhelms the heart, in which case CO levels off. Therefore, within the physiological limit
of the heart, the followingqualitative constraint holds:
M+(CVPM, CO)
50
Heterometric & Homeometric Autoregulation of the Heart
When the cardiac muscle becomesstretched an extra amount, as it does when extra amounts
of blood enter the heart chambers, the stretched muscle contracts with a greatly increased
force, thereby automatically pumping the extra blood into the arteries. This ability of the
heart to contract with increased force as its chambers are stretched is sometimes called
heterometric autoregulationof the heart.
Furthermore, when the heart is stretched, changes in heart metabolism cause an additional increase in contractile strength. It takes approximately 30 seconds for this effect to
develop fully, an effect called homeometric autoregulation [11].
Therefore, within the physiological limit of the heart, the ventricular contractility (VC)
of the heart increases with the stroke volume (SV):
M+(SV, VC)
Effect of Heart Rate on Cardiac Output
An increase in heart rate can be caused by a higher oxygen demand in tissues and organs,
as in physical exercise, or as a compensatory mechanism for a decreased arterial blood
pressure, as in hypovolemia. In general, the more times the heart beats per minute, the
more blood it can pump, as long as the stroke volume stays roughly the same. This can be
seen from the equation
CO = HR x SV
Therefore, if the stroke volume does not decrease, or if the decrease in stroke volume is
more than compensated by the increase in heart rate, the followingqualitative constraint
holds:
M+(HR, CO)
Indeed, a rise in heart rate increases the net influx of calcium ions per minute into the
myocardial cells, and enhances ventricular contractility:
M + (HR, VC)
This increased contractility causes blood to be pumped out faster from the ventricle,
51
shortens the systolic interval, allocates a larger proportion of the cardiac cycle to diastolic
ventricular filling, and therefore maintains the stroke volume at a reasonable level.
However, once the heart rate exceeds a critical level (150-170 beats per minute in normal
individuals), the heart strength itself decreases, presumably because of overutilization of
metabolic substrates in the cardiac muscle:
M-(HR, VC)
This results in a significant decrease in diastolic filling time and consequently a decrease in
the stroke volume:
M- (HR, SV)
The tolerable limits for heart rate decrease with underlying cardiovascular impairment.
For example, ventricular tachycardia in a patient with recent myocardial infarction produces
a significant reduction in stroke volume, cardiac output, and subsequently arterial blood
pressure also [11, 42].
Compensatory Mechanisms for Hypovolemia
Hypovolemia refers to an absolute and often sudden reduction in circulating blood volume relative to the capacity of the vascular system [32]. The major homeostatic defense
mechanism in hypovolemia is activation of the sympathetic nervous system. The signal for
activation of increased adrenergic nervous activity is decreased cardiac output and systemic
arterial blood pressure.
A decline in systemic arterial blood pressure and/or blood vol-
ume activates stretch baroreceptors in the aortic arch, carotid sinus, and splanchnic arterial
bed. Volume-sensitive baroreceptors within the heart can also be activated. Increased signals from these baroreceptors to the central nervous system lead to increased sympathetic
nerve efferent responses and decreased parasympathetic activity. This triggers a series of
compensatory mechanisms including:
* arteriolar vasoconstriction with resultant decreased perfusion to skin, skeletal muscle,
kidney, and splanchnic organs. This causes an increase in the skin-to-core temperature
gradient AT:
M-(CO, AT)
52
* tachycardia:
M- (CO,HR)
* increased rnyocardial contractility:
M- (CO, VC)
53
Chapter 5
System Architecture
5.1
Overview
The goal of the learning system is to generate qualitative models from physiological signals.
The overall architecture of the system is illustrated in Figure 5-1.
Figure 5-1: Overall architecture of the learning system.
The physiological signal is first processed by a front-end system, which outputs a filtered
signal and its derivative. These are entered into the segmenter to produce a qualitative
behavior in terms of a set of qualitative states. GENMODEL then uses this qualitative
behavior to generate a qualitative model. 1
This chapter describes the front-end system and the segmenter in detail. GENMODEL
is described in Chapter 3.
5.2
Front-End System
The architecture used for front-end processing of physiological signals is shown in Figure 5-2.
The signal first passes through an artifact filter which removes various artifacts and
linearly interpolates the intervals of the artifacts removed. The resulting signal is then
1
The front-end system and the segmenter are implemented in Objectworks\Smalltalk on the HP9000/720.
54
Incoming Signal
x[n]
y[n]
y'[n]
Processed Signal
Derivative Signal
Figure 5-2: Architecture used for front-end processing of physiological signals.
processed by a median filter which removes impulsive features lasting shorter than half the
length of the filter window. A Gaussian filter then smooths the signal to the desired level
of temporal abstraction by convolving it with a Gaussian kernel of an appropriate standard
deviation a. Finally, this smoothed signal is passed through a differentiator to obtain its
derivative. The smoothed signal and its derivative are passed on to the segmenter for seg-
mentation, producing a set of qualitative states describing the system behavior represented
by the signal.
The Gaussian filter and the differentiator are implemented as finite impulse response
(FIR) filters. For simplicity, the same length L is used for the median filter window and the
impulse responses of the Gaussian filter and the differentiator. Also, since we are interested
only in the qualitative behavior represented by the signals, and not in the absolute magnitudes, certain constant factors in the impulse responses have been omitted for simplicity.
2
2
With a filter length of L, the filters require , points before and after the current point to process
each point. In processing the first and last L-1 points, we extrapolate the signals by repeating the first and
last values beyond the beginning and the end of the signals respectively. This way, the processed signals are
of the same length as the original signals.
55
F
eEi
20-
· o
40
5o
I- i .
So
70
I
80
.
90
100
- ·'I
110
120
i
30
im·/
Figure 5-3: An artifact found in blood pressure signals, caused by flushing the blood pressure
line with high pressure saline solution.
f
m
Tim/.
Figure 5-4: An artifact found in blood pressure signals, caused by blood sampling from the
blood pressure catheter.
5.2.1 Artifact Filter
Physiological signals from hemodynamic monitoring contain various kinds of artifacts which
are due to clinical interventions, hardware faults or other causes, rather than real patient
conditions. The artifact filter removes these artifacts and linearly interpolates the intervals
of the removed artifacts.
Figures 5-3, 5-4 and 5-5 show three types of commonly encountered artifacts. These and
many other types of artifacts are roughly intervals during which the signal abruptly rises
(drops) to an abnormally high (low) value. Therefore we can achieve reasonable performance
in our artifact filter by adopting a simple threshold approach. When the magnitude of a
signal rises above a certain threshold which cannot be physiologically attained in general,
the filter removes the abnormal values and interpolates the interval with the last normal
value. This approach of detection and interpolation is relatively simple in nature, and may
not work well for signals with complex artifacts or artifacts of long durations.
For recognition of complex artifacts, a knowledge-based system can be used. [12] describes a blackboard system for artifact recognition in blood pressure signals. [18] describes
56
N ___ - ___- _
-
I1001
i
r
t
F-
°-O-..
6
-I1 O-
I
s-
-1
--
-J50
I
L
i
I
I
Tim./.
Figure 5-5: A general artifact caused by the transducer being left open to air.
a neural network approach for the same problem.
5.2.2
Median Filter
The median filter operates by centering a window of a given length L at each point of the
signal, as shown in Figure 5-6.
The output at that point is the median of the values covered by the window. The
median filter is therefore a non-lineartime-invariant filter. It removesimpulsive features in
the signal with durations less than half of its window length, while retaining sharp edges
of remaining features. (Unlike filters based on convolution, the median filter outputs only
values existing in the input signal. It does not produce any new averaged values.) This
property of the median filter makes it useful for removing short impulsive artifacts in the
physiologicalsignals prior to smoothing by the Gaussian filter. This prevents the impulsive
artifacts from distorting the smoothed signals.
5.2.3
Temporal Abstraction
A complex system such as the human cardiovascular system involves processes operating at
different time scales. From the same set of signals, depending on the particular time scale
we are interested in, different sets of qualitative states and therefore different models can
be obtained.
In [21]Kuipers describes a temporal abstraction relation among mechanisms operating
at significantly different time scales. Processes that occur significantly faster than the time
scale of a model can be considered as instantaneous in the model, while those that occur
much slower can be considered as constant.
For example, if we look at a system on the
order of hours, processes that occur within milliseconds can be considered as instantaneous,
57
Impulsive noise
(duration = 2)
x[n]
r
70
4
l4 I
7
50
4
I
Feature with sharp edge
(duration = 5)
4I 1 4lII
1
I
W
4
___
_
WW
W
-
-
W
_
-
-
_
_
W
W
0 10 170170o
-
-
--
-
~_
w
w
1
_
n
W
1
1
0I
0
o1501505
window length = 5
I
I
10i0701701
dian0 70170
00I olsol
sorting
sorting
0 0
median = 50
median = 0
Features with duration < 3
are filtered.
MEDIAN FILTERING
y[n]
Sharp edge retained
50
I
D4
4
4
4I
Impulsive noise filtered
u
h
W
W
M
____
W
W
W
l
W
W
W
W
W
W
_____
w W
n
Figure 5-6: The median filter removes features with durations less than half of its window
length, but retains sharp edges of remaining features.
58
while those occurring over days can be viewed as constant. Therefore if we perturb a system
by increasing a function A, and observe that another function B responds to this change
within milliseconds by increasing its value, then we can still model the relationship between
A and B with the functional constraint M+(A, B) even though there is a delay between the
perturbation
and the response, since the response within milliseconds is seen as occurring
instantaneously at this time scale.
We incorporate this idea of temporal abstraction into our learning system by the following scheme:
1. First, we use a Gaussian filter to remove changes lasting significantlyshorter than the
time scale we are interested in. This is described in Section 5.2.4.
2. Next, we implement the segmenter in such a way that critical points of different
functions occurring within r sampling periods are labelled as occurring at the same
distinguished time point, where the parameter
corresponds to the particular time
scale at which we are interested in learning. This is described in Section 5.3.
Without the first step, there is a danger of aliasingin the temporal abstraction process.
Features lasting for short durations (< -) can be aliased into one lasting for a long duration.
This issue is described in the following section.
Aliasing
We mentioned that temporal abstraction is incorporated into our learning system by means
of the Gaussian filter and the segmenter. In particular we described the parameter r of our
segmenter which controls the degree of temporal abstraction allowed in the segmentation.
Upon reaching a critical point in one of the system functions, the segmenter searches the next
r points in the signals of the other functions, looking for critical points. The segmenter then
labels the critical point of the initial function together with all other critical points found in
the remaining functions as occurring at the same distinguished time point. Therefore in the
subsequent stage when GENMODEL learns from the qualitative behavior generated by the
segmenter, a function Y which always responds monotonically with the function X within
a delay of r sampling periods can be included in the constraint M+(X, Y) or M-(X, Y).
In fact, since the segmenter labels the different quantitative times as the same distin-
guished time point, the delay has been abstracted from GENMODEL. GENMODEL cannot
59
tell from the qualitative behavior given to it by the segmenter whether a delay has occurred
or not.
However,if we omit the Gaussian filter and retain features lasting significantly shorter
than r sampling periods, there is a danger of aliasingin the temporal abstraction process.
Features lasting for short durations (< r) can be aliased into a feature lasting for a long
duration. In Figure 5-7 the signal g(t) is distorted into h(t) by aliasing. g(t) contains two
impulsive features at t = 100 + 6 and t = 200 + 6. Both of these features begin and end
within the temporal abstraction time . Since each feature is associated with a critical
point and the segmenter regards all critical points that occur within -r to occur at the same
distinguished time point, the feature at t = 100+
and t = 200 + a cause the signal to
be labeled as steady at the critical points g(1) and g(2) respectively. The segment between
t = 100 + r and t = 200 + r is labeled as decreasing from g(1) to g(2) according to its two
endpoints. Therefore g(t) takes on the identity (alias) of h(t) in the qualitative behavior
produced. Consequently, the incorrect monotonic constraint:
M+(f, g)
is learned in the subsequent stage.
The aliasing we observe in the segmentation of signals (i.e. a quantitative-to-qualitative
conversion) is analogous to the aliasing observed in the sampling of continuous signals (i.e. a
continuous-to-discrete conversion). If a continuous signal is sampled at a frequency less than
the Nyquist rate (i.e. 2N where LQNis the highest frequency within the signal), without
first passing the signal through an anti-aliasingfilter which removesthe Fourier components
whose frequencies exceed
AQN,these
Fourier components will be distorted into signals with
frequenciesless than fQN,which will then add to the originally existing components at those
lower frequencies and corrupt the signal in a non-recoverable way [26]. This is analogous to
the way features with durations significantlyshorter than r corrupt the qualitative behavior
produced upon segmentation if we had omitted our anti-aliasing Gaussian filter.
5.2.4
Gaussian Filter
The idea of using a Gaussian filter to analyze changes in a signal at different scales is borrowed from the well known technique of scale-space filtering in edge detection. Scale-space
60
<f(O),inc>
f(t)
<f(O)/f(1),inc>
f(300)=(100) ---------------
<f(l), std>
<f(O)/f(1),dec>
<f(1),std>
<f(O)/f(1),inc>
<f(1),inc>
..
-
f(0) = f(200) 0
f(l)
10~-,
0160
200
200+
landmark
value
f()
t
<g(O),inc>
g(t)
g(300)="g(100)
-- -----
<g(O)/g(1),inc>
1
10aa
f
<h(O),inc>
fl
nn
n _= | n-lrv
nk.I=
ntvu = nul
g(1), stdi
<g(O)/g(1),dec>
<h(O)/h(1),inc>
t
<h(1)i std:
2
<h(O)/h(1),dec>
200+
11.
i00
100+
r-------..-------
200
I
t(1)
-------------------
I
.LI")
300 "tI
200+%
20048
100+8
t(O)/t(1)
g(O)
ch(1)j std> <h(O)/h(1),inc> <h(l), inc>
----------------------
-----------------------------------------
0
g(l)
g
_
---
t(O)
std> <g(O)/g(l), inc> <g(l), inc>
.g(1),
-
g(0) = "g(200)"
h(t)
,
t
t(2)
t(1)/t(2)
t(2)
t(2)/t(3)
t(3)
distinguished time point
Figure 5-7: The effect of aliasing in the segmentation of a signal with the temporal abstrac-
tion parameter set to r. g(t) is aliased into h(t) in the qualitative behavior produced.
61
filtering constructs hierarchic symbolic signal descriptions by transforming the signal into
a continuum of versions of the original signal convolved with a kernel containing a scale
parameter.
In an image, changes of intensity take place at many spatial scales depending
on their physical origin. Marr and Hildreth [23] observed that detecting zero crossings in
the Laplacian of the intensity values across different scales enables a system to distinguish
between a physical edge from surface markings or shadows. They suggested that the original
image be bandlimited at several different cutoff frequencies and that an edge detection algorithm be applied to each of the images. The resulting edge maps have edges corresponding
to different scales.
In our learning system, we need to segment a set of signals at different time scales. We
can do so by bandlimiting our original signals at several different cutoff frequencies and
segmenting the signals by detecting zero crossings in the first derivative of the signals at
different scales. The segmentation then produces a set of qualitative behaviors at different
time scales which can be given to GENMODEL to produce qualitative models at different
scales.
To bandlimit an image at different cutoff frequencies, the impulse response of the lowpass
filter proposed by Marr and Hildreth is Gaussian shaped. This choice is motivated by the
fact that the Gaussian function is smooth and localized in both the spatial and frequency
domains. 3 A smooth impulse response is less likely to introduce any changes that are not
present in the original shape. A localized impulse response is less likely to shift the location
of edges. Further, Yuille and Poggio [43] and Babaud et al. [1] have separately shown that
the Gaussian filter has a unique property concerning zero crossings of the first derivative of
the filtered signal: 4 moving from coarse to fine scale, new zero crossings appear, but existing
ones never disappear. Consequently, the extrema can be used to construct a tree describing
the successive partitioning of the signal into finer subintervals as new zero crossings appear
at finer scales. This partitioning of the signal by extrema moving from coarse to fine scale
forms a strict hierarchy. Scale-space filtering in edge detection can be seen as a form of
the more general technique of wavelet transforms in multiresolution signal analysis, with
the wavelets here being Laplacians of shifted Gaussians, and signal edges located by zero
3
The Gaussian function has the smallest duration-bandwidth product with duration and bandwidth as
defined in [33], and is therefore optimally localized in both the time and frequency domains.
4In general, this property holds true for zero crossings obtained by applying any linear differential operator
(including the Laplacian and the first derivative) to the filtered signal.
62
crossings of the wavelet transform [35].
We adopt a similar approach for segmenting our signals. The impulse response of the
lowpass filter used is based on the Gaussian function:
g(t) =
1
t2
e 2
for -oo < t < oo and a > 0. The standard deviation a determines the cutoff frequency
with a larger a corresponding to a lower cutoff frequency. a therefore determines the time
scale we are operating at, with a smaller a corresponding to a finer time scale and a larger a
corresponding to a coarser scale. The frequency response of the lowpass filter is the Fourier
transform of g(t) which is also Gaussian shaped:
G(Q)
e
n2,2
2
To translate this into a discrete-time filter, we simply replace t with n, yielding g[n] as
follows:
g[n]=
1
n2
,e
2
for -oo < n < oo and a > 0.
To obtain a finite impulse response (FIR) h[n] from the infinite impulse response g[n],
we multiply g[n] by the Hanning window w[n]:
h[n] = g[n]w[n]
where
[] 0.5 -
.cos( 2r(n+2)
M
<<
M
otherwise
0
This avoids the nonuniform convergence (the Gibbs phenomenon) associated with abrupt
truncation of an infinite impulse response [26]. The Hanning window w[n] is plotted in
Figure 5-8. In our experiments, we used values of a at 10, 20, 40, 60, 80 and 100. h[n] is
plotted as shown in Figure 5-9 for these values of a.
M is the order of the FIR filter. Therefore M + 1 is the length of the impulse response:
L=M+1
63
n
Figure 5-8: Plot of the Hanning window w[n].
0.02
A
0.018
[
.:a=20
.. :a=40
-. :a=60
-:=80O
-: a= 100
1.
:
0.016
0.014
0.012
0.01
0.008
0.006
1,'
0.004
0.002
-00
-200
-100
0
100
200
300
n
Figure 5-9: Plots of impulse responses h[n] of Gaussian filters for a = 20, 40, 60, 80, 100.
64
Ia
M(=6a)
10
20
40
60
80
100
60
120
240
360
480
600
L(=M+
1)
61
121
241
361
481
601
Table 5.1: Table showing the orders M and lengths L of the Gaussian filters corresponding
to a = 10,20,40,60,80,100.
.:=20
:.~
0.9
-. :a=60hO
!,*
0.6
'
,,-:
= 100
0.7
0.6
'0.5
0.4
:I't
0.3
·I
0.2
i
.'''I
..
0.1
-. 08
-0.06
-0.04
-0.02
'
0
0.02
0.04
0.06
0.08
A1.
Figure 5-10: Plots of frequency responses H(Q) of Gaussian filters for a = 20,40,60,80, 100.
In our learning system, M is set so that the finite impulse response extends to three standard
deviations from the origin:
M
-=
3a
2
which yields:
M =6
Table 5.1 shows the lengths and the orders of the filters that correspond to the six values
of a we used in our experiments:
The frequency response H(Q) is Gaussian shaped as shown in Figure 5-10 for the six
values of a used in our experiments.
65
0.8
0.8
0.4
0.2
-0.2
-0.4
-0.8
-0.8
-300
i
-100
-200
0
100
200
300
Figure 5-11: Impulse response of an FIR bandlimited differentiator.
5.2.5
Differentiator
The differentiator is implemented as an FIR filter based on the frequency response of a
bandlimited differentiator [26]:
H(e- '
) =
jw -7r < w < r
The corresponding impulse response is:
h[n]=
n
o
rnosrn-sinrn
_ 00
<n <
7rn7--~--- -Cx <
< cx
=0
fn
0O
h[n]=
cosrn
o
n540
n
This infinite impulse response is multiplied by the Hanning window to obtain a finite
impulse response hd[n] as shown in Figure 5-11. The frequency response of this FIR bandlimited differentiator is shown in Figure 5-12.
It is interesting to note that the lowpass filtering operation of the Gaussian filter and
the derivative operation of the differentiator may be combined to obtain a single filter with
the derivative of the Gaussian function as its impulse response:
t
vJ27r
,
66
t2
WY~
Figure 5-12: Frequency response of an FIR bandlimited differentiator.
0.035
.: o = 20
.. :=40
-. :a=60
0.03
-:a=0
0.025
._0.02
-0.015
0.01
0.005." .
'
''
'
"
Figure 5-13: Equivalent frequency responses of a Gaussian filter in cascade with a bandlim-
ited differentiator for a = 20,40,60,80, 100.
The corresponding frequency response is as follows:
G'(Q) = je
02,2
2
This frequency response is plotted in Figure 5-13.
From the frequency response, we note that the combined operation is equivalent to
bandpass filtering where a controls the bandwidth of the bandpass filter. Bandlimiting
the signals tends to reduce noise, thus reducing the noise sensitivity problem associated
with detecting zero crossing points.
With increasing values of a, the bandwidth of the
bandpass filter decreases and therefore more noise rejection is achieved. This agrees with
our expectation since larger values of a correspond to coarser time scales.
67
2E
To
III
.r
i
I"
AI
Figure 5-14: A segment of the mean arterial blood pressure (ABPM) signal. Note the
artifacts at t = 600, 1000, 3400 seconds.
So
Time/s
Figure 5-15: The ABPM data segment processed by the artifact filter. Note that the
artifacts have been filtered but the signal contains many impulsive features.
5.2.6
An Example
Here we show a segment of mean arterial blood pressure signal (Figure 5-14) and show the
signal as it passes through the
1 artifact filter (Figure 5-15), the median filter (Figure 5-16),
the Gaussian filter (Figure 5-17), and the differentiator (Figure 5-18). In this example, the
length of the filters used is 61, i.e. L = 61.
5.3
Segmenter
The segmenter consists of two parts: a function segmenter for each function of the system,
and a qualitative behaviorgenerator to coordinate the whole segmentation process. The
overall scheme is illustrated in Figure 5-19.
The function segmenter segments each signal at zero crossings of its derivative obtained
68
E
E
I
I
a
r-
I
...
.. I
. ...
.... .
500
I .... .
1000
.
I
1500
2000
2500
l
3000
..
-
3500
Time/$
Figure 5-16: The ABPM data segment processed by the median filter. Note that the
impulsive features have been filtered.
E
E
2I
I
I
I
.9
-6
.r
i
I
0
500
1000
1500
2000
2500
3000
3500
Time/s
Figure 5-17: The ABPM data segment processed by the Gaussian filter. Note that the
signal has been smoothed.
I,
E
E
:8
It
II
E
RI
I
I
2
-6
.C
2
-k
I
E
Time/s
Figure 5-18: The ABPM data segment processed by the differentiator.
69
Distinguished
Time
Point
Qualitative
Function
State
t(7)
x(t(7),x(4)/x(l),inc)
Qualitative Behavior
Generator
Instance Variables:
Disting. Time Point List
Temporal Abstraction
QualitativeSystemState
(x(t(7),x(4)/x(1),inc),y(t(7),y(7),std),z(t(7),z(4),dec))
Figure 5-19: Overall scheme of segmentation to produce a qualitative behavior from processed signals and derivatives.
70
from the differentiator. It then looks up its local landmark list to see if there is any existing
landmark within a tolerance from the current value of the function. If so, the existing
landmark becomes the qualitative value of the function in this state. If not, the segmenter
creates a new landmark corresponding to the current value of the function, returns this
landmark as the qualitative value of the function in this state, and stores the new landmark
in the local landmark list. The direction of change of the function in the current state is
obtained by observing the sign of the derivative. A positive derivative corresponds to inc
(increasing). A negative derivative corresponds to dec (decreasing). A derivative within a
tolerance from zero corresponds to std (steady). The qualitative value and the direction of
change together form a qualitative state of the function.
The qualitative behavior generator keeps track of distinguished time points and coordinates the entire segmentation process. When any one or more of the function segmenters
detects a zero crossing in their derivatives, the generator waits for r sampling periods to
see if any other segmenters also detect a zero crossing in their derivatives. The parameter
- therefore determines the level of temporal abstraction, as discussed in Section 5.2.3. 5
The generator labels all times within these r sampling periods as the same distinguished
time point. It then signals all segmenters to segment their signals at this time point. The
generator then collects a qualitative state of each function from its segmenter, and combines the qualitative states of all the functions of the system into a qualitative state of the
system at the current distinguished time point. A series of such qualitative states form a
qualitative behavior of the system. This is written into a text file for subsequent input into
GENMODEL.
5r is set to M = 3 so that the corresponding frequency Q2=
is well within the cutoff region of the
lowpass Gaussian filter. This avoids the aliasing problem discussed in Section 5.2.3.
71
Chapter 6
Results and Interpretation
The learning system was applied to data segments obtained from six patients during cardiac
bypass surgery. 1 A data segment from each of the first five patients was used to study how
qualitative models learned vary across patients. Six data segments from the same patient
(Patient 6) during the same surgery were used to study how qualitative models learned
vary within a patient.
The models learned are compared with the cardiovascular model
described in Section 4.2.
Each data segment was 1000 seconds (16.7 minutes) long, sampled at 1 Hz. The fault
tolerance level in GENMODEL was set at 20% of the total number of qualitative states in
each data segment. The operation performed in each case was to insert coronary artery
bypass grafts, except in the case of Patient 2 which was to replace the aortic valve. Models
were learned from the data segments at six different levels of temporal abstraction, represented by the six different values of L as shown in Table 5.1 in Section 5.2.4. The results
are described below. For each data segment, a brief overview of the patient's condition is
given, followed by a plot of the original signals. Then the filtered signals at each of the six
levels of temporal abstraction is shown followed by the model learned and an interpretation
of each of the model constraints.
'Raw data was recorded from the HP Component Monitoring System at a local hospital. The eight
parameters used for the experiments were derived from these primary measurements as described in Section 4.1.
72
6.1
Inter-Patient Model Comparison: Patients 1-5
6.1.1
Patient 1
The patient was a 39-year-old gentleman with familial hyperlipidemia syndrome and a 3-4
year history of angina. Upon cardiac catheterization,
he was found to have widespread
triple vessel coronary artery disease but a well functioning left ventricle. He was on calcium channel blockers, beta-blockers, aspirin, GTN (glyceryl trinitrate or nitroglycerin, a
vasodilator) and a drug to control his hyperlipidemia.
Prior to the interval corresponding to the data segment, lightness in anesthesia caused a
rise in ABP following skin incision from 109 mmHg systolic to a peak of 137 mmHg systolic.
During the interval, the anesthetic (Enflurane) was increased and a bolus of analgesic (2
ml of Alfentanil) was administered to dampen the response to surgical insult and avoid
myocardial ischemia. The ABP was subsequently brought down.
.
4nn
i
4n_
i
i
lVV
r
m 80
-
- ____III I
5
r
Fill
i
o00
I-
I
1000
1500
2000
goo
1000
t/sec
1000 -
UU
I 100
oo
1500
2000
t/sec
VI II
1000
1500
C>
500
III
00
2000
.
.
rrrmarrmrru
1000
t/sec
1500
2000
1500
2000
t/sec
X 10 5
5
01
O~>a
T-If
LA&---------1'11
o00
1500
1000
-500
2000
t/sec
t/sec
X 10 4
a-
-1
kal -
u
500
I
_'.I j -A-
IIaJ
w0
-
I
1000
1000
1500
2000
90
t/sec
t/sec
Figure 6-1: Patient 1: Original Signals. Note the relatively constant heart rate due to the
effect of beta-blockers.
73
-7
/
Il
co 60
C-· A
C
2a-
6
Q.
L
00oo
Jl
1000
1500
2000
-
IL
500
goo
1000
t/sec
100
I
__
·
1500
500 -
·
80
-
> 400
T'
"'
0--41!
"~oVo
'
1500
1000
'00
2000
t/sec
2000
1000
1500
2000
1500
2000
1500
2000
t/sec
t/sec
x 1)04
5 -
0
o
C)
oo00
1000
1500
1
g0
2000
1000
t/sec
t/sec
nAnn
I i lf "
"
lI-
I-
a
a. 8000n'
6000 -
500
1.
·a
I .
I-J 1.4
LU
0
1500
1000
2000
i
4
5'00
1000
t/sec
t/sec
Figure 6-2: Patient 1: Filtered Signals (L = 61)
L=61
.No constraints were obtained.
74
70-
!
3,4
~~~~ ~ ~
>L 6
60
z[
50o)0
1000
1500
I
500
2000
1000
t/sec
80
·-
.51
1000
1500
1000
2000
1500
2000
t/sec
x 104
4-
jiu
.II
1000
1500
_
oo
2000
--------i
1000
t/sec
10000
v500
500
.....
t/sec
.
.
-
a0
. 8000
cc
..
1500
IIB
"oo
2000
/sec
0(
2000
Cn400
'goo
4.5
1500
.1 II
I
I IIvv
-·
2000
rnn_
nn _
I
1500
t/sec
Q- 1.6 -
i
w
1000
1500
2( )00
t/sec
1.4
1.2
500
1000
t/sec
Figure 6-3: Patient 1: Filtered Signals (L = 121)
L=121
mult(HR, ABPM, RPP) (Correct)
mult(HR, SV, CO) (Correct)
75
iB
"I
·
it
7
0
1000
1500
2000
oo00
1000
t/sec
CTI
1500
2000
1500
2000
t/sec
Arn
100
> 400
r--n
an
""'
-'hql
VToo
1000
1500
l'
2000
1000
t/sec
84
4
3.5
3.&I II
.
cr
I
1
II
2
I .. ..
·
1000
1500
·
ii i·
1000
1500
!00
2000
t/sec
2000
t/sec
4
..
L- I.V
.
8000
1
·
o1
0
00
a
t/sec
-
1 .4
500
o
1000
1500
0
I
2( )00
I 5000
t/sec
1000
1500
2( 100
t/sec
Figure 6-4: Patient 1: Filtered Signals (L = 241)
L=241
M+(ABPM,
RPP)
Correct given that HR was constant due to beta-blockers.
increased due to increased Enflurane dosage.
mult(HR, ABPM, RPP) (Correct)
mnult(HR, SV, CO) (Correct)
76
ABPM
71n
IIIX
<a
7
Iv
60
0
u
-
/--/-
I
-1
'goo
1000
1500
2000
1000
t/sec
100
I-r
13:
Jl
80
rn 1
.
1500
2000
2000
1500
2000
1500
2000
-
1000
-. goo
t/sec
t/sec
4.5rX 104
2
4.
01.
4
I
' o0
1000
1500
2000
1000
t/sec
t/sec
x
1500
_
n=^
.s
2000
>3 400
1000
00
1500
t/sec
nnnn
I,
I UUUU
a
- 8000
E:
]f · 1
Ln[ Jli[
w
500
1.4
0
-
I
1000
1500
2000
t/sec
1.
J
--
.0
50
500
1000
t/sec
Figure 6-5: Patient 1: Filtered Signals (L = 361)
L=361
M- (ABPM, VC) VC increased to compensate for decreasing ABPM due to increased Enflurane dosage.
mult(HR, ABPM, RPP) (Correct)
77
"7
!7
Iu
E-6
60
oI_
"
1000
1500
2000
1000
goo
t/sec
80
_
-
1500
2000
1500
2000
1500
2000
1500
2000
t/sec
·
la
Arn
~1
a_
I.v
I
tr
m 70
400
=n _
-goo
·
1000
65 0
tsec
1500
2000
1000
Vsec
4
y 1,v
4.2 1 '
0o
z
4
1-
&R~-0
A
1000
1500
.
2000
1000
t/sec
t/sec
I----n_
IllllI
Ill
I- 1.6
I UUVVVV
a-
a.
Cc 8000
5 1.4
w
Ernnn
.1 II BI
500
1000
1500
.
4 ni -
I
2000
t/sec
_
500
1000
t/sec
Figure 6-6: Patient 1: Filtered Signals (L = 481)
L=481
M+(ABPM,
RPP)
Correct given that HR was constant due to beta-blockers.
increased due to increased Enflurane dosage.
M+(CVPM, VC) Both increased - Frank-Starling Law of the Heart.
M-(ABPM, SV) (Spurious)
M- (SV, RPP) (Spurious)
mult(HR, SV, CO) (Correct)
78
ABPM
70
7_
f-
-
n 60
a 6
500
1000
1500
"8
2000
1000
o00
t/sec
z
70
-I- ""'
:1!'1
1000
1500
L -,'
0o
1000
x1
I
nI
oo
2000
1500
2000
i~~~~~~
II
1000
1500
.
!00
2000
1000
t/sec
t/sec
xrnnrn_
I BB BI BB]
1 1
IVVI
t-
13 8000
n
l1a
Ern
v.vgoo
.B .
1500
Vsec
4
."
a
2000
I'
2000
t/sec
"
1500
> 400
---
___
o.o
2000
.
ApJ'
.LL
z
.
1500
t/sec
..
W
.. .I
1000
1500
I .u
1.4~
I
2000
t/sec
.
'
500
1000
t/sec
Figure 6-7: Patient 1: Filtered Signals (L = 601)
L=601
M+(ABPM,RPP)
Correct given that HR was constant due to beta-blockers.
increased due to increased Enflurane dosage.
M+(CVPM, VC) Both increased - Frank-Starling Law of the Heart.
M+ (HR, CO) Both decreased because of increased Enflurane dosage.
invderiv(ABPM, RPP) (Spurious)
inv_deriv(ABPM, VC) (Spurious)
mult(HR,ABPM, RPP) (Correct)
mult(HR, SV, CO) (Correct)
79
ABPM
6.1.2
Patient 2
The patient was a 65-year-oldblind and partially deaf lady who was admitted in acute left
ventricular failure and found to have significant aortic valve regurgitation. The operation
performed was to replace the patient's aortic valve and to check a mitral valve installed
approximately 27 years ago.
The data segment was taken when the patient was just coming off bypass and was
artificially paced.
4 nn
I
I V
IE
2
50
CD
0
.I
I
9000
9500
10000
10500
9o600
_
k_
9500
i/sec
Jl
M 100
-Iz zi r
I
LII
Trrr-L
n
·
-I
9000
9500
10000
9000
10500
9500
i/sec
x 106
10000
·
10
IL JL
0
E
n-'Y·1
· YU~y-.
i
-=h
9500
·
~·YI·
i
10000
-900
10500
9500
t/sec
10000
10500
i/sec
-x 104
'V
4I
a
JI--
Er
-J
w
0
9500
10500
t/sec
·
-1
9000
10500
x 104
-n
Cv
10000
i/sec
10000
In
"6oo
10500
9500
10000
10500
t/sec
i/sec
Figure 6-8: Patient 2: Original Signals. Note the relatively constant heart rate due to
artificial pacing.
80
^A
"All
Jl
c.
_
> 10t
m
0
r
9ooo00
500
·
9500
n,
Y..-
1000_
7$y--
,..
9500
10000
...
9'0o
900
10500
t/sec
00
X 104
i-
rv _
9500
10500
10000
10500
10000
10500
_
10000
10500
9ooo00
9500
t/sec
t/sec
"IB "
n
I- "
.
i
L
n~
J.u
'
m
I-; 0.6
nE 8000
-J
0 nA [
I
6000-
10000
t/sec
IB
9500
9ooo00
nn
I
II
·
0 0.5
5
I
I
U, 500
i75
10
10500
t/sec
Vsec
'9o00
10000
9500
10000
10500
9600
inn
9500
t/sec
t/sec
Figure 6-9: Patient 2: Filtered Signals (L = 61)
L=61
M+(SV, CO) Correct given that HR was constant due to artificial pacing.
mult(HR, SV, CO) (Correct)
81
/~s
Ar,
35
50
i-
m3
000oo
9500
10000
n_
0
5j9000
10500
9500
10000
10500
10000
10500
10000
10500
10000
10500
t/sec
t/sec
800
I-r- 78
> 600
(0 -o
JII·II BI
900o
9500
10000
'100oo
10500
t/sec
9500
t/sec
4~~o°
x 104
r
0o 6
U> 0.5
9000
-vv'
i iq
9500
10000
10500
9'000
9500
t/sec
9000
a.
n
n-
-
t/sec
·
-0.8 0.6
8000
0
7000
9000
9500
10000
10500
0.4
9000
t/sec
9500
t/sec
Figure 6-10: Patient 2: Filtered Signals (L = 121)
L=121
M+(SV, CO) Correct given that HR was constant due to artificial pacing.
82
55
·
·
Jr., _
m
rn 50
> 4_
0
,-I
4!
93000
^
/_//
·
·
9500
10000
105500
9500
t/sec
10000
10500
t/sec
0OU
800_
78
60 0
II
.
.
-
OO_
·· _
I7'9 00
Jl III
9500
10000
I I
9000
10500
9500
Vsec
10000
10500
10000
10500
Vsec
4
,X 10
4i .
II
0 0.5
06
AII _
!
-1
9000
9500
10000
10500
90ooo
9500
t/sec
9000
-
t/sec
0.8
.
.
a.
a 8000
0.6
_VO
i
I VVV
I.......
.
.
-
9000
w
III ~rll
9500
10000
_
9U i00
10500
t/sec
9500
10000
t/sec
Figure 6-11: Patient 2: Filtered Signals (L = 241)
L=241
M+(SV, CO) Correct given that HR was constant due to artificial pacing.
83
10500
_'
-i
-
50
aC2
t
4
1j.
§-oo
9500
10000
_
9000
10!500
9500
t/sec
80
700
.
.
78
'9'600
9500
10000
1.
.
.
9500
10000
10500
10000
10500
10000
10500
t/sec
I
_
9%00
0 0.5
.l
9500
10000
9'00
10500
9500
t/sec
t/sec
..
| .no
V...-
8000
AL
a-
7nA
.
.
900
,x 104
o6
-
500
10500
t/sec
I
10500
i 600
--lm
J
10000
t/sec
0-J
" 'A
_
, vv
9000
0.6
9500
10000
10500
IL
''6oo
t/sec
9500
t/sec
Figure 6-12: Patient 2: Filtered Signals (L = 361)
L=361
No constraints were obtained.
84
A_
U
2 50
4
,
j,
900
9500
10000
10500
900oo
t/sec
m
9500
9EvD
fUU
I 78
10000
10500
/sec
.
.
j 650
9000
9500
10000
l I I
t
w9ooO
10500
.
9500
t/sec
2
.
.
10500
t/sec
104
7x
.
10000
.
.
C
I6
,1
Il
9o00
9500
10000
10500
9o00
9500
t/sec
n-OUUU
10500
10000
10500
0.8
0-
a.
Ir
10000
t/sec
0.6
nn
J ~
IIB
Wa
0C.n
__
9000
9500
10000
10500
i JA
_
_
Vo00
t/sec
9500
t/sec
Figure 6-13: Patient 2: Filtered Signals (L = 481)
L=481
No constraints were obtained.
85
·
0 -
2
2
50
6o
o000
9500
10000
9'00
10500
9500
t/sec
10000
10500
10000
10500
t/sec
7n..
III
80
78
Cn650.
'9000
9500
10000
,n.^
9VooO
10500
9500
t/sec
t/sec
14
I
·
.
.
o6
I
9000
9500
10000
I
10500
I
9000
9500
t/sec
10500
10000
10500
t/sec
nnn
II
·i · I
...
aa-
10000
OvVV
i
w 0.6
a:
-Inn
a
I
9000
9500
10000
..n .A
_
9000
10500
t/sec
9500
t/sec
Figure 6-14: Patient 2: Filtered Signals (L = 601)
L=601
M- (ABPM, SV) (Spurious)
86
6.1.3
Patient 3
The patient was a 47-year-old gentleman who had a recent large myocardial infarction and
recurrent episodes of left ventricular failure since then.
His exercise tolerance was very
poor and he developed a left ventricular aneurism following the myocardial infarction. The
operation performed was insertion of coronary artery bypass grafts and excision of the
ventricular aneurism.
The data segment was taken when the surgery was just starting.
4n_
lBtI.
n
80
0-
0
o
1000
1500
LLSU-·Y"
·
1000
2000
i/sec
I
WU -
aI
0
1 1Eli
_UU9660
rY
1000
1500
2000
1500
2000
i/sec
2000
·
-
0-
,
W.'pi IL.
----
'.......
1500
'WVVKo
0
2000
1000
t/sec
/sec
x 105
d~
I E B
IV
ILI.
,..L--
0-500
1000
1500
0
0
O.1
2000
-
-
I
'oo00
1000
t/sec
1500
2000
1500
2000
MJ,
0
11.5i
04
!
1500
II
t/sec
x 10 4
1000
I W l-1
I
--
/ L- J
i
500
2000
1000
t/sec
t/sec
Figure 6-15: Patient 3: Original Signals
87
7r I -
to,
m 60
500
50;
1000
1500
2000
t/sec
4
2 500
1000
1
.
> 300
'1
200
500
t/sec
L
x 134
._
113~~~~~~
sX
1500
2000
1500
2000
1
° 0.5-
n
v
__ I
500
·
1000
1500
'iSy
I~~~~~~
2000
500
t/sec
H 2
5000
5000
1
.
1000
1000
t/sec
10000
II
lJ
1000
t/sec
02
o
0-
2000
400
I
a
1500
t/sec
1500
2000
t/sec
O_
500
.
.
1000
1500
t/sec
Figure 6-16: Patient 3: Filtered Signals (L = 61)
L=61
No constraints were obtained.
88
2000
70II I
co 60
·
2a.
0
_
4 i/
n- 9
Ern
500oo
1000
1500
2000
500
1000
t/sec
400 -
100
IX
2000
.
.
> 300
0---JII
1000
1500
BI
'"oo
2000
1000
t/sec
4
x 104
1500
t/sec
1000
t/sec
11
"
aaa: 5000
1
uJ
!
1000
1500
2000
I
!
00oo
I
I
1000
1500
t/sec
t/sec
Figure 6-17: Patient 3: Filtered Signals (L = 121)
L=121
M + (HR, RPP)
2000
Bi
oo
2000
nnnr
0-
1500
0 0.5
i
500
2000
_
I
1000
BlBB
"I
1500
t/sec
32
(D
B
1500
t/sec
Correct due to slowly rising ABPM.
mult(HR,ABPM,RPP) (Correct)
mult(HR, SV, CO) (Correct)
89
2000
70 -
>4
a- 60
EL
co
I
O
rn.
1000
oo00
1500
2000
500
1000
t/sec
1500
2000
1500
2000
1500
2000
t/sec
70
barn
6JDU
I 60-
> 300
T
r- n --
500
1500
1000
2000
1000
t/sec
I
I
1
t/sec
X 1 ()4
4_
]r
(>)0
00 23
yo1
-
12
1000
5oo
1500
2000
o00
1000
t/sec
Onnf
J
uv- ]]
~l
t/sec
_
.¢'
a_
a- 6000
n'
4000 -
500
5i--
·
·
1000
1500
0
·
2000
500
t/sec
1000
1500
t/sec
Figure 6-18: Patient 3: Filtered Signals (L = 241)
L=241
AM+(HR, RPP)
Correct due to slowly rising ABPM.
mult(HR, ABPM, RPP) (Correct)
nmult(HR,CVPM, RPP) (Spurious)
,mult(HR, SV, CO) (Correct)
90
2000
70
a. 4
60
L
rEn
-oo
0
.
.
1000
1500
0
1000
0oo
2000
,,
/U
400
3 60
> 300
[
500oo
1000
1500
2000
1500
2000
1500
2000
t/sec
t/sec
1500
ok4 )O
sV0
2000
------/
1000
t/sec
t/sec
x 104
1
0
>0.5
O 2
t
_
II
oo
1000
1500
goo
2000
1000
t/sec
annnII
I
t/sec
eII
I
a
L 6000
4000 500
- 1
0
I
1000
1500
!
500
2000
1000
1500
t/sec
t/sec
Figure 6-19: Patient 3: Filtered Signals (L = 361)
L=361
mult(HR,ABPM,RPP) (Correct)
mult(HR, SV, CO) (Correct)
91
2000
'=
·
/U
6
2
·
a-4
60
O
i
...
-~l!
|
ffi
1000
1500
2000
1000
t/sec
7^
2000
1500
2000
400 -
/U
C> 300
60
cn
Inn
'oo
_
-III
5'oo
1000
1500
2000
I~
I
1000
/sec
ex
t/sec
104
1
0 0.5
02
i
1500
t/sec
I--
i
500
1000
1500
OL
0
2000
1000
t/sec
I
1500
2000
1500
2000
i/sec
8000
H 1.5
f-
6000A1~1 ^Ill
LU
a
1
500V
500
1000
1500
2000
iJ i
r,
_
500
t/sec
1000
t/sec
Figure 6-20: Patient 3: Filtered Signals (L = 481)
L=481
M+(HR, RPP)
Correct due to slowly rising ABPM.
92
9
6
aa. 60
a
0
o00
1000
1500
4
--
(
1000
2000
t/sec
70
400 -
1500
2000
t/sec
.
.
>c 300
I
JII
1000
1500
2000
'
1000
oo
t/sec
10)4
,x
Li
0 0.5
02
I
1000
1500
2000
1000
t/sec
1.EIr
·
0 6000
1
C \r
I
V.0
5
AAlto
II IB
1000
1500
2000
2000
_
1000
t/sec
i/sec
Figure 6-21: Patient 3: Filtered Signals (L = 601)
L=601
M + (HR, RPP)
1500
f
I
0-
500
2000
t/sec
c
8000 -
III
1500
t
I
I
go 0
2000
1
.
.
1500
/sec
Correct due to slowly rising ABPM.
mult(HR,ABPM, RPP) (Correct)
93
6.1.4
Patient 4
The patient was a 60-year-old gentleman with a history of angina and breathlessness on
exercise.
He had been a non-insulin dependent diabetic for many years.
His coronary
angiography showed severe triple vessel disease with an occluded right coronary artery and
severely impaired left ventricular function. He was on beta-blockers (Atenolol) and calcium
channel blockers (Nicardipine).
The data segment was taken when the operation had just started, and the period was
relatively uneventful.
1 \~m~ ·
aco 70
8
0
IwFn#ljvI
cJ
1500
1000
2000
2500
1500
1'600
t/sec
-1·
rn
2500
nrnr
'JII
- 100
L,,,,1, ,,,, ,
n
100oo
I
2000
t/sec
I·
Al
lf00
, A
111TAP"
BI
1500
tsec
2000
1000
2500
1500
2000
2500
t/sec
,,x 105
o_
.I- -kill.
Ii
IAMI
ULWL
'I'T'F7TrIq7rrI1TWi"7
1500
1000
J
L&dIdlILL..
2000
·
_c.
2500
1000
1500
t/sec
Ax
z
tsec
2000
2500
104
a 1-
0-
II.
1.-L I
1000
nFTL .
4~u1LLJX
1500
2000
a 1.5
10002500
1000
t/sec
1500
2000
2500
t/sec
Figure 6-22: Patient 4: Original Signals. Note the relatively constant heart rate due to the
effect of beta-blockers.
94
11
a
eo
100
1500
2000
0 6_
2500
o000
1500
t/sec
4hi Or
-44
*
,
.
800
.
1500
2000
8000
2500
1500
t/sec
x 10
0
0
2000
2500
900
c)
A-
2500
I UUU-
:
I
1000oo
2000
t/sec
t/sec
4
1
.
.
J.i
0>0.5
AI
fl
1000
1500
2000
2500
1ib00
1500
t/sec
2000
2500
2000
2500
t/sec
""'
rcnn
_
I
4·
a.
a- 5000n
4500
1000
w
0
1500
2000
2500
J
q
B
_
1 boo
t/sec
1500
t/sec
Figure 6-23: Patient 4: Filtered Signals (L = 61). Note that the trends of the relatively
constant heart rate are amplified.
L=61
No constraints were obtained.
95
i/\i
n.
M
·
6CI.I
a:
"`
'i000
1500
2000
44 l
G"
A,1
ZL.4
__
1o00
1500
2000
~~~~ ~ ~
6
C
A
2500
L
10 0
t/sec
AC
··-
!
a
n'n iii
900
M
2500
I...
2000
2500
2000
2500
t/sec
vJ
VVI
.B.
(n
1500
1500
100
t/sec
t/sec
x 104
0 0.5
00 5
·
Z
1000
1500
2000
25 00
1000
1500
t/sec
PA
I
II
1 .,II
11
2500
So
w
0
...
1000
2000
I
I-
5000
I~.
2500
t/sec
rRt5
O--IL
2000
1500
2000
2500
4
I
I
b 00
110
t/sec
1500
t/sec
Figure 6-24: Patient 4: Filtered Signals (L = 121)
L=121
M+(SV, CO) Correct given that HR was constant due to beta-blockers.
M+(CVPM, /T) (Spurious)
mult(HR, SV, CO) (Correct)
96
6.
oh><.
i
" 56
0
ED
c··
1500
0boo
2000
2500
,_ .
1000
150
1500
o-
44
i/V
&
Z3."
i000
1UUU
|
w
l
!
2500
2000
·
900
(
nr--
!
1500
2000
t/sec
t/sec
III
nl
'too
2500
t/sec
1500
2000
2500
2000
2500
2000
2500
t/sec
x 104
U
0C 5
0 0.5
it
nA!I
1oo00
1500
2000
2500
1000
1500
t/sec
t/sec
-- nn
c'
[.013.5000
I[
w
1.·
.J.IJVV
0
1
~1
1"00
1500
2000
2500
1
boo
1500
t/sec
t/sec
Figure 6-25: Patient 4: Filtered Signals (L = 241)
L=241
M+(CO,RPP) (Spurious)
M+ (SV, CO) Correct given that HR was constant due to beta-blockers.
M+ (SV, RPP) (Spurious)
mult(HR, SV, CO) (Correct)
97
6.5 1
Q- 57
a
6
13
C
.
100
1500
2000
2500
00
5
.
1500
t/sec
2000
2500
t/sec
non _u
..IVVV
......
I
C0 900
Inn
... ii.
u1oo
A1
00oo
1500
2000
2500
1500
2000
2500
t/sec
t/sec
x 10
(. 0.5
85
0
!
100
1500
2000
1000
2500
1500
t/sec
2000
2500
t/sec
,,
ac""""
1.
.
.
DUO
L 5000
I--
-
uJ
w
0
_
1000
I
1500
2000
2500
i
t/sec
b000
1500
2000
t/sec
Figure 6-26: Patient 4: Filtered Signals (L = 361)
L=361
M + (SV, CO) Correct given that HR was constant due to beta-blockers.
mult(HR, SV, CO) (Correct)
98
2500
6.5
r
E
m 57-
CC7 _
1000
/
1500
2000
.
.
6
I
1i000
2500
1500
t/sec
2000
2500
2000
2500
t/sec
xrnnn
I
I III
I vIU
I 44.5
>) 900
arn_
AA ,
~1
1500
1000
2000
2500
III.
1000
1500
t/sec
t;c
t/sec
x 104
0 0.5
00-
5
4 -
1000
_-
.
·
1500
2000
2500
1000
t/sec
rri
Ir
5000
A-n
Jl
"l
2000
2500
2000
2500
t/sec
rnn
JJUU
a0
.
1500
I- 1.5
_
1000
1000
uJ
w
0
1
I
1500
2000
2500
I
__
Iboo
10
00
t/sec
1500
t/sec
Figure 6-27: Patient 4: Filtered Signals (L = 481)
L=481
rmult(HR, SV, CO) (Correct)
99
57
a-)
O
Gc
1000
1500
2000
2500
6
L
1 000
1500
t/sec
2500
.nn
I UUU
AZI
> 900
r44.5
no
--
AA
·
0)~r!I
I
1000
1500
2000
1000
2500
1500
t/sec
2000
2500
2000
2500
2000
2500
t/sec
1
x 104
O 0.5
0) 5
Jl
2000
t/sec
AI
1000
1500
2000
1000
2500
1500
t/sec
t/sec
r Ann
0Q
0- 5000
aI
A
Jl
"1
UJ
0
An
1000
1500
2000
2500
4
i
t/sec
B
boo
1500
t/sec
Figure 6-28: Patient 4: Filtered Signals (L = 601)
L=601
mult(HR, ABPIM, RPP) (Correct)
mnult(HR, SV, CO) (Correct)
100
6.1.5
Patient 5
The patient was a 66-year-oldgentleman with a fairly long history of angina and a proven
inferior infarct 3 months before the operation. He had very poor exercise tolerance, developing severe ischemia after very moderate exercise. His catheterization showed severe triple
vessel disease with reasonably good left ventricular function. He was hypertensive and was
treated with beta-blockers (Atenolol). He was also a non-insulin dependent diabetic.
The data segment was taken quite some time after the surgery had started. Before the
period, the initial lightness of anesthesia caused a sharp rise in ABP from 90 mmHg systolic
up to 160 mmHg systolic and that was sustained for several minutes. During the period,
the depth of anesthesia (Enflurane) and analgesia (Alfentanil) and the dosage of GTN were
increased to bring the ABP back down.
80
·
-
1
2a.
m 60
C)
":
An
gl
Ill
_
'o0(
3500
0
4000
4500
30
t/sec
I'll
Jtc--
r
I.
I III
I
i/sec
_
et3
:s0oo0
I
4000
!
!
-
-;·C
I
3500
X 104
3'000
4500
·
3500
t/sec
106
-x
I
·
·
I
3000
3500
-B
4000
4500
4000
4500
t/sec
·
5
>r,
S
4000
4500
3000
t/sec
3500
t/sec
x 104
a
Ec
0
- -r
-J
_,^
C3
!
3000
3500
4000
4500
30
t/sec
t/sec
Figure 6-29: Patient 5: Original Signals. Note the relatively constant heart rate due to the
effect of beta-blockers.
101
2a-
A
60
50
3
0
40
300
3500
4000
4500
3'boo
t/sec
zir
1
3500
'1I IIIBI
nn
7:
.hh1
300
__
I
·
3500
4000
·
II
4500
3ooo00
3500
t/sec
x 104
1
o0
4500
.
.
> 0.5
ll
I
30ooo
3500
4000
_
3600
4500
3500
t/sec
---I
I VVV
.
a- 6000
rnn _
...
4000
t/sec
-1
cc
4500
> 500
iiri--?
Jl
4000
t/sec
3--0
II
is-\
300( 0
3500
4000
4500
4000
4500
t/sec
4000
2.2
4500
3000
t/sec
3500
t/sec
Figure 6-30: Patient 5: Filtered Signals (L = 61). Note that the trends of the relatively
constant heart rate are amplified.
L=61
M-(CVPM,
AT) (Spurious)
M+(SV, CO) Correct given that HR was constant due to beta-blockers.
M+(CVPM, AT) (Spurious)
102
"I
n.l
50
a0
n
A
Jlm
Fr
:
a;3- C
-
|
3500
-3o00
I
I
3500
4000
4500
4000
4500
4000
4500
4000
4500
^~~~~~
4000
3000
4500
t/sec
._
__
bV
I
t/sec
600
·
I
300(0
-\
> 400
-ii7
""
l
nnhl_
3500
4000
-Jl I 1
LUUv
4500
3000
3500
t/sec
t/sec
x10 4
1
t.
oO 4
> 0.5
,
A
J
3000
3500
4000
4500
3v00
3500
t/sec
7000 0-
- 6000
mnn
..
-
|
t/sec
w
\N
\
L 2.2
UJ
JJ..J
300JU_
300( 0
3500
4000
4500
3000
t/sec
3500
t/sec
Figure 6-31: Patient 5: Filtered Signals (L = 121)
:L=121
.No constraints were obtained.
103
0u
-
·
·
·
·
I
Im
an 50
co
0
3000
3500
0
4000
4500
-
-
3500
3'b00
I.3000
> 400
4000
3500
---V
onn I
4500
3oo000
·
·
3500
4000
tsec
x104
1
·
0 0.5
0
I
3000
3500
4000
3'o00
4500
!
3500
4000
4500
4000
4500
Vsec
t/sec
·
-
- 6000
w
(r --I
4500
t/sec
04
7000
4500
600
60
a5
I 58
6
4000
t/sec
t/sec
2.2
0
II
VVUV
3000
3500
4000
4500
3000
3500
t/sec
t/sec
Figure 6-32: Patient 5: Filtered Signals (L = 241)
L=241
M+(SV, CO) Correct given that HR was constant due to beta-blockers.
mult(HR, SV, CO) (Correct)
104
I
f!
<I
4
·
·
"3.
CL-
50
30(
·
al
3500
oo
4000
4500
i
)0
3500
t/sec
,,
600
·
·
'30000
3500
4000
40030( )0
4500
I
3500
Vsec
104
0.5
A
901DO
3500
4000
4500
_
3vo00o
0
!
3500
t/sec
-
a-
4500
1
0
35
4000
t/sec
4
7000
·
> 500
U58
0
4500
t/sec
·
4.5
4000
4000
4500
t/sec
·
·
·
·
-
I-r 2.2
- 6000
w
0
5000
300C
3500
4000
4500
.
3000
t/sec
.
3500
4000
4500
t/sec
Figure 6-33: Patient 5: Filtered Signals (L = 361)
L=361
M+(ABPM, HR) (Spurious)
M+(ABPM,
RPP)
Correct given that HR was constant due to beta-blockers.
dropped because of increased depth of anesthesia.
M+ (HR, RPP) (Spurious)
M+(SV, CO) Correct given that HR was constant due to beta-blockers.
rmult(HR,ABPM, RPP) (Correct)
rmult(HR,CVPM, RPP) (Spurious)
mult(HR, SV, CO) (Correct)
105
ABPM
60
4-
-
m 55.
·
·
3
-
^
S
3500
5300
4000
300
4500
·
·
3500
4000
60
8'g
4500
t/sec
t/sec
600 -
E
·
·
> 500
1 58
"'A^O
3000
3500
4000
4500
"o00
3500
t/sec
x 104
I'
I.
4500
4000
4500
1
_
00 t4.
',
4000
Vsec
0 0.5
iI
o7000
3500
4000
4500
3'000
3500
t/sec
t/sec
7000 -
·
- 2.2
w
LJ
a. 6000
5000
·
-
3000
·
3500
4000
4500
3000
t/sec
·
3500
4000
4500
t/sec
Figure 6-34: Patient 5: Filtered Signals (L = 481)
L=481
A+ (ABPM, RPP)
Correct given that HR was constant due to beta-blockers.
ABPM
dropped because of increased depth of anesthesia.
M-(ABPM,
VC) VC increased to compensate for decreasing ABPM due to increased
dosage of anesthetic, analgesia and GTN.
M- (RPP, VC) (Spurious)
mult(HR, ABPM, RPP) (Correct)
106
"I
A
11 r
u_
rm 55
n I
~1
h1UC
>C
I
3500
30003
4000
3'00
4500
3500
t/sec
^A I
Lred,
nlJ
58
N
58
4000
4500
4000
4500
> 5000
300o
3500
4000
4500
/11
nn
I
3000
3500
t/sec
X 10
4500
600-
·
_
l
4000
t/sec
t/sec
4
,,
0o
(> 0.5
4
O
or
soc
iii
3500
4000
4500
3000
3500
t/sec
7nrnn_
I
t/sec
I-
a- 6000
2.2
5000
300( 0
0
I
3500
4000
4500
I
3000
t/sec
3500
4000
4500
t/sec
Figure 6-35: Patient 5: Filtered Signals (L = 601)
L=-601
M+(ABPM,HR) (Spurious)
M+(ABPM,
RPP)
Correct given that HR was constant due to beta-blockers.
dropped because of increased depth of anesthesia.
.M(CVPM, CO) Frank-Starling Law of the Heart.
.M4(HR, RPP) (Spurious)
nmult(HR,ABPMI, RPP)
(Correct)
mrult(HR, CVPA1, RPP) (Spurious)
mnult(HR, SV, CO) (Correct)
107
ABPM
6.2
Intra-Patient Model Comparison: Patient 6, Segments
1-6
The patient was a 63-year-old gentleman having 1 internal mammary artery and 3 coronary
artery grafts. He had a history of 6 years of hypertension, 4 years of angina and 20 years
of chronic bronchitis. His angiogram showed well presented left ventricle, totally occluded
right ventricle and severe disease at the origin of all left sided vessels. He was not on
beta-blockers.
6.2.1
Segment 1
Previous to this segment, lightness in anesthesia caused rises in ABP (up to 180 mmHg systolic) at leg surgery, chest incision and sternotomy. The patient then developed myocardial
ischemia. In response to this, the GTN dosage was increased, which along with hypovolemia
caused the ABP to drop, with the result that ischemia improved at the expense of blood
pressure. The depth of anesthesia was also increased.
150
4
·
I
a.
. 100.
0
G--
1000
55oz
0
1500
2000
n
1v;
I
_
'0
-100 _
I
1000
500
i/sec
1500
cnn
III
.1
5000 -
I.1VV
0
cr
X
-111\
l ..
-5000 -
. .
1000
-"oo00
1500
--1W.,.III,
I 6-1-
0-
cn
--
2000
500
1000
t/sec
0
2000
i/sec
4x r
|
106
2000
5_LL..iL.L
( 0
1500
/sec
i...--
alh.
Ir1- lr nr'
--
mI·-
-oo
1000
1500
2000
1000
t/sec
104
Px
J.~
a.e 0
2
aU
in3
UIUIIIYrUIJIU*;
_-11l
500
2000
1500
2000
1-4
w: -
I
I
1500
t/sec
I
1000
1500
2000
oo00
t/sec
-
I.
1000
t/sec
Figure 6-36: Patient 6, Segment 1: Original Signals
108
nn_ I
r
I III
iVV
CL
M:
50
-)
O
L
A
1500
1000
0oo
0okO
-o00
2000
71
1|
1000
2000
1500
2000
nnn
100
III
I VUv
> 500
50
l' -
I
goo
|
|
1000
1500
\·
goo
2000
1000
t/sec
t/sec
10
1500
t/sec
t/sec
x 10
14
ie
I
1000
goo
1500
1000
2000
1500
2000
x 104
\
500
0
2000
t/sec
t/sec
2
1500
500
_
U3
1000
1500
wD
1
2000
500
1000
t/sec
t/sec
Figure 6-37: Patient 6, Segment 1: Filtered Signals (L = 61)
L=61
mult(HR, ABPM, RPP) (Correct)
109
5
100
a
.
.
a- 0
O3
.)
'~ 1000
"o00
1500
2000
_
-;
500
.
2000
1500
2000
1500
2000
1500
2000
Ir-nr
III I.
II
I
I
1UU
cc 50
I
C>
L
500
iii
goo
1000
1500
2000
r
goo
1000
t/sec
t/sec
x 104
10
0o
1500
t/sec
t/sec
rrrr
II
,
IUV
.
1000
14
i r
, 0.5
5
_
II
n _
I I,
0oo
1000
1500
2000
goo
1000
t/sec
j-I-
t/sec
x 104
aa1
Cn
00-500
1)
50 2-
iri1000
1500
2000
500
t/sec
1000
t/sec
Figure 6-38: Patient 6, Segment 1: Filtered Signals (L = 121)
L=121
'rlult(HR, ABPllI, RPP) (Correct)
mult(HR, SV, CO) (Correct)
110
100
>
r
0
0 I_
50s0
1000
1500
2000
-o00
Iv
1500
2000
t/sec
-n
·· ·
1000
t/sec
1000
> 500
50
A
00oo
n
5o 0
·
1000
1500
2000
·
1000
2000
1500
2000
1500
2000
tsec
Vsec
4
1500
104
1
0.5
2
I
0oo
!
0
1500
1000
2000
1000
t/sec
t/sec
_
n'' 1·04
a
a13 1r-
2
0.
LU
.
I
vU
500
1000
1500
2000
I
_
goo
1000
t/sec
/sec
Figure 6-39: Patient 6, Segment 1: Filtered Signals (L = 241)
L=241
M-(HR, SV) (Spurious)
inv-deriv(ABPM, RPP) (Spurious)
invderiv(ABPM,
VC) (Spurious)
111
_nr
,....
Ivv
0
a.
U
a-
m
_
c,\
'goo
..
1000
1500
500
2000
1000
1500
2000
1500
2000
1500
2000
1500
2000
t/sec
t/sec
100
4 ffnnn
I
....
Ivvv
50
u) 500
l-
I
1000
goo
1500
500
2000
1000
t/sec
t/sec
X 104
4
1
0(D
o 0.5
n
0oo
1000
1500
2000
00oo
1000
t/sec
fx
t/sec
10 4
e·
a
a- 1
n
2-
A1L
500
q
1000
1500
2000
I
_
goo
t/sec
1000
t/sec
Figure 6-40: Patient 6, Segment 1: Filtered Signals (L = 361)
L=361
M + (HR, RPP) Both dropped because of increased depth of anesthesia.
mult(HR, ABPM, RPP) (Correct)
mult(HR, SV, CO) (Correct)
112
A
·4El nnlI
I UV
a.
>2
M
n,
...
0
__
-
oo
1000
1500
2000
0
1000
t/sec
1500
2000
t/sec
100 -
1000
I 50
> 500
I
1000
o60
1500
1000
2000
Vsec
1500
2000
Vsec
4
10
I!
0
82
>0 0.5
III
II
oo00
1000
1500
2000
500
5
I
I
1000
1500
20 00
1500
2000
t/sec
t/sec
4
x o10
I
J
a.
1
0
I.
C.,4·-
.
500
I~~~~~~~~~~~~~~~~
1000
1500
oo
2000
t/sec
1000
i/sec
Figure 6-41: Patient 6, Segment 1: Filtered Signals (L = 481)
L=481
M + (HR, RPP) Both dropped because of increased depth of anesthesia.
M+(ABPM,
AT) Both dropped because of vasodilating effect of GTN.
invderiv(ABPM, RPP) (Spurious)
inv deriv(ABPM, VC) (Spurious)
mult(HR, ABPM, RPP) (Correct)
mult(HR, ABPM, VC) (Spurious)
mult(HR,CVPM,RPP) (Spurious)
mult(HR, SV, CO) (Correct)
113
11Il1
4-
_rr
I UU
L
a-
2
m
1
n
I,
IJ90)
I
1000
1500
2000
o00
1000
100
2000
1500
2000
1500
2000
1500
2000
UU -
a:
I 50
I!
1500
t/sec
t/sec
> 400
206-
I'
1500
1000
2000
1000
t/sec
t/sec
4
n x 10
4_
I-
o 0.5t
II
I I
III
g00
1000
1500
00
2000
1000
t/sec
t/sec
,x 104
m
_
!a1
1
'-
, I
500
1000
1500
2000
500oo
t/sec
1000
t/sec
Figure 6-42: Patient 6, Segment 1: Filtered Signals (L = 601)
L=601
t+ (ABPM, CO) Both dropped because of vasodilation and increased venous tone caused
by increased GTN dosage.
M + (HR, RPP) Both dropped because of increased depth of anesthesia.
M + (ABPM, AT) Both dropped because of vasodilating effect of GTN.
IM+(CO,AT) Both dropped because of vasodilation and increased venous tone caused by
increased GTN dosage.
invderiv(ABPM, RPP) (Spurious)
invderiv(ABPM, VC) (Spurious)
mult(HR,ABPM, RPP) (Correct)
mult(HR,CVPM,RPP) (Spurious)
mult(HR, SV, CO) (Correct)
114
6.2.2
Segment 2
The increased GTN dosage successfully lowered ABP and improved ischemia. In this segment, GTN dosage was reduced.
80
-
r
>
a211*uun~~unrIII
~~~~~~
m 60
rn
IL 4
L---
I
2000oo
2500
"'fij
0D
3000
V~
t/sec
An-
ii I i
500 An
JfiJ
ZUL
I
10(
I
Fiji
.1 1,..
)
APW
U
.. .. .
2500
I,.,~..
2000
3000
10
.1
.
3
0
>C -
2oo00
2500
-
ri
-r
3000
'ooo
t/sec
x 10
nI
C
2(500
- - -
-
,7
Onr11
2500
t/sec
30100
C
1. ,4TJ
II
3000
2500
t/sec
t/sec
x
,L111~1
_-
200UU
..
2( 000
00
3000
2500
b0oo
t/sec
LL.
2500
t/sec
1.
Ff
1
3000
4;nl
200
i
2500
t/sec
Figure 6-43: Patient 6, Segment 2: Original Signals
115
30(30
60
c
50 >
AN
0
C-
illI
,l'l
I, ....
2500
t/sec
3000
o00
2500
3000
t/sec
1000
I
,,vv
szj7C
I 50
,I
'"
2v00
2000
Il
2
15
_
2000
2.5
> 500
r
A'00
%
2500
t/sec
!
3000
-x 1(4
2500
t/sec
3000
2500
t/sec
3000
2500
3000
2
0U
I
1
2000
I
"v
A
2500
t/sec
---A
,I~1111E
II II III
Q. 5000
2000
20C00
I-- 1.2
r
iii
[
2v-
3000
L- 1.1
w
---
0
·
2500
t/sec
3000
4i
_
2b00
t/sec
Figure 6-44: Patient 6, Segment 2: Filtered Signals (L = 61)
L=61
mult(HR, SV, CO) (Correct)
116
vuv
...
__
·
~~~~~~~~~~~~~~~~~2.5
0EL
- 50
2
O
An
--
2000
.~~~~~~~~~~~
2500
t/sec
15
3000
ZO00
n,
I
I~
IUU
1000
50
> 500
'1
2500
t/sec
3000
2500
t/sec
3000
2500
3000
A
00
2500
t/sec
2O 90
20(
3000
Ax 104
2
4 r
01 I-
o
O22
i
i !
II
2d00
2500
2000
30i 00
t/sec
t/sec
100( U
cc
|
5 00 -
,
1 .0
- 1.1
\
2000
2500
30100
12_
20( 0O
t/sec
2500
t/sec
Figure 6-45: Patient 6, Segment 2: Filtered Signals (L = 121)
L=121
M+ (HR, RPP) Correct given relatively constant ABPM.
mult(HR, ABPM, RPP) (Correct)
117
3000
hi
2.5
f
a-
50
<c
20oo
2500
t/sec
3000
2
0 IE- =
'' oo
2500
t/sec
3000
2500
30 00
1000
uv
Ic
T 40
> 500
nIl _
'200oo
2500
3000
2600
/sec
A
/sec
x 10 4
_.-__
i
1.5
02
0
c
1
n l
I!
2500
t/sec
2000
I-_-
3UUU
3000
t/sec
I
.
L
0r
w
2000
2500
t/sec
~~~~~~~~~~~~~~~~~~~~~
2500
30 00
ooo
3000
\-1-
1.1
1!
--
2b00
.
2500
t/sec
Figure 6-46: Patient 6, Segment 2: Filtered Signals (L = 241)
L=241
deriv(SV, CO) (Spurious)
118
3000
>
'L
Cl
2.5
2
50
O
2500
t/sec
2000
3000
I 5,
'00oo
3000
t/sec
hl\h
60
I UUU
I 40\
> 500
r%
~Ct
2500
t/sec
3000
20(30
00 2
0
|
2i 00
600( II=
1
n -1
,
.
2500
t/sec
:oo
3000
2500
- 1.2
0 400(
r
-* 1.1
-
-
-
w
0
2500
3000
t/sec
-
200C I
2( 00
3000
m
·
.1
1
_
_
2500
t/sec
X 10 4
,__
_
.,
2500
3000
1
!
2b00
t/sec
-
~
2500
t/sec
Figure 6-47: Patient 6, Segment 2: Filtered Signals (L = 361)
L=361
'mult(HR, SV, CO) (Correct)
119
-
3000
I
J
>
a-
co 50
It
2
0o
c-l
_,
B
0oo
2500
t/sec
'oo
3000
.4I nfrf
.....
n- 40
T'
c 500
_
2500
t/sec
n
2v0(00
3000
21
1
.,
2500
t/sec
2C)00
I--
n0-
4000
n
l~~~~~~~~~~~~~~~~~~~
2500
t/sec
3000
I"
oo
u2U000
3000
l~~~~~~~~~~~~~~~~
2000
3000
1.5
0
o 2
2000 -
2500
t/sec
x 104
6000 -
3000
l B
B
2VOI
00
2500
t/sec
60
on
t
!
4
i
2500
t/sec
3000
2500
t/sec
3000
I
1.1
.4
B
2b00
Figure 6-48: Patient 6, Segment 2: Filtered Signals (L = 481)
L=481
nM+
(HR, VC) Both were relatively steady.
deriv(SV, CO) (Spurious)
120
rr
55
~~ ~
~
~
~
~
~
~
~
~
2.
am 50
2
E
>
_
AC
2000
_ _
_
_
_ _
_
0 4
_
2500
t/sec
I__
3000
'200
2500
t/sec
3000
2500
t/sec
3000
2500
t/sec
3000
2500
t/sec
3000
f'n
--
Du
I UW0
> 500
:40
on
00
2500
t/sec
n
2'000
3000
1
x 104
j2
O
_.
co2
A>r
2000
2500
t/sec
u60o
3000
---- nx
a.
a 4000
-
1= n
1.1
LU
2500
t/sec
2000
3000
2b00
Figure 6-49: Patient 6, Segment 2: Filtered Signals (L = 601)
L=601
M+ (HR, RPP) Both continued to drop because of increased depth of anesthesia.
1M-(ABPM, HR) ABPM started to rise moderately following decreased GTN dosage.
M- (ABPM, RPP)
ABPM started to rise moderately following decreased GTN dosage.
deriv(SV, CO) (Spurious)
mult(HR, ABPM, RPP) (Correct)
mult(HR, ABPM, VC) (Spurious)
mult(HR,CVPM,RPP) (Spurious)
mult(HR, CVPM, VC) (Spurious)
121
6.2.3
Segment 3
The patient condition was stabilized. Depth of anesthesia was decreased. This period was
uneventful.
QU
a.
0
4
1 .
a.
70
0 ,imnflM]bhII
iJlnlyrJlj\/i*N*-J/JC/C
3500
i/sec
0ooo
4000
3500
3bl00
4000
t/sec
Annr.
20
UUUVV
100
> 2000
~.L.
_..L...,.
=.. _
n II,'
n1111
3500
i/sec
3V00
4000
3'600
.
AL. J AM
.
-~,~.
~.A.
3500
t/sec
40100
x 105
4I
0
02
A,
tr~~~~ulr~~A11
0
b-
3500
4000
3'000
t/sec
4
I'
4
4
I.
-
a.
rI
3ooo00
I.
I
I-
6.1
w0
rd
3500
3500
40100
t/sec
X 104
n
Ir
.I..
-
3600
a- 1I
I
4000
I
'3600
t/sec
3500
t/sec
Figure 6-50: Patient 6, Segment 3: Original Signals
122
40100
r
ml I li
2.
r
Z.b
2
>
2
_
4
3500
t/sec
'300
4000
1I nn
3500
t/sec
4000
3500
t/sec
4000
3500
4000
nnnrr
I UU
I-v
I 50T"',
> 500
n
I m _
I! I'
3500
t/sec
3v000
4000
a300
104
1U I
0o-
1
_-
5
o 0.5
-
Il I
30(00
II ll
l VVVV
c 5000
CC
Ai
S~~~~~~~~~~
3500
t/sec
II
4000
t/sec
-r
3r00
3v000
1. I r
-H
I-
0
3500
t/sec
4000
1 1 =
3000
3500
t/sec
Figure 6-51: Patient 6, Segment 3: Filtered Signals (L = 61)
L=61
mult(HR, ABPjM, RPP) (Correct)
rmult(HR, SV, CO) (Correct)
123
4000
Fij
20 I
a 54
&J
in,
2
01I
!
3500
0oo
4000
.
'3000
4
100
V
> 500
n1
I!
3ooo00
*.l lI
3500
3oo00
4000
tsec
4000
1
o 0.5
5
n
I
remN
I
I!
3Vooo
3500
4000
3oo00
t/sec
3500
4000
t/sec
Iv
100CEn
a.
a
3500
t/sec
x 104
1u I
o
4000
nn
1II
I
50
0
3500
t/sec
t/sec
4,..
ro
I-
500)0
1
-L
3'6000
3500
4000
t/sec
1.1 =
3000
3500
t/sec
Figure 6-52: Patient 6, Segment 3: Filtered Signals (L = 121)
L=121
M- (CVPM, AT) (Spurious)
M + (HR, RPP)
Both rose because of decreased depth of anesthesia.
mult(HR,ABPM, RPP) (Correct)
mult(HR, CVPM, RPP) (Spurious)
mult(HR, SV, CO) (Correct)
124
4000
11~~~~~~~~nL
"I
00
- ---p
t.0
54
A6
'300
4000
'3000
i/sec
3500
4000
i/sec
-~r
I--1uuu
u
50
-
I
1 ri
3500
> 500
A
n
3'000
3500
4000
300
t/sec
3500
4000
t/sec
x 104
4
IV
o 0.5
05 'U
n
n
3000
3500
4000
3V000
t/sec
3500
I
4000
t/sec
4I AAAA
-
0V
I-
f- 5000
A
A
2
0
3000
3500
4000
3000
t/sec
3500
t/sec
Figure 6-53: Patient 6, Segment 3: Filtered Signals (L = 241)
L=241
M + (HR, CO) Both rose because of decreased depth of anesthesia.
M+(RPP, VC) Both rose because of decreased depth of anesthesia.
mult(HR, ABPM, RPP) (Correct)
mult(HR, CVPM, RPP) (Spurious)
mnult(HR, CVPM, VC) (Spurious)
mult(HR, SV, CO) (Correct)
125
4000
_IIA
r-.I.
53 ~-
>.
'-
rI
'3000
1 no
u
C,
Ui
n X 10
4000
_
*Il
3500
t/sec
3500
t/sec
50,
I
·
4000
o
n
rooo
-
2
0
3500
t/sec
3000
-
I
-I
r I3
I
50 D
40100
3 30oo
3500
/sec
4000
4
1
0
>0.5
(D 5
I!I
300oo
3500
t/sec
40100
i
3'000
3500
t/sec
4000
3500
4000
II nnn
on
1I Ilil
uuuq
a.
0
)
I2r
0/l
500( D
III
i
I
ri
i1
33000
3500
40 DO
3000
t/sec
t/sec
Figure 6-54: Patient 6, Segment 3: Filtered Signals (L = 361)
L=361
M+(CO, RPP) Both rose because of decreased depth of anesthesia.
AM+(HR, CO) Both rose because of decreased depth of anesthesia.
M + (HR, RPP)
Both rose because of decreased depth of anesthesia.
mult(HR, ABPM, RPP) (Correct)
mult(HR, ABPM, VC) (Spurious)
mult(HR, CVPM, RPP) (Spurious)
mult(HR, CVPM, VC) (Spurious)
mult(HR, SV, CO) (Correct)
126
r
2.EIh
f a ll.
r
m
53
I
_
ob00
rrrI
I
2
i
3500
t/sec
4000
U '3000
> 500
50
A\
_
300
3500
4000
03_
'00
tsec
I
3500
40 00
t/sec
.n_
0(D
4000
1000
IrV
···
.11
i
3500
t/sec
I
JUU
I
02a. 1 r, _
X 104
1
0 0.5
0
n
i I
300oo
3500
40100
3ooo00
3500
4000
t/sec
t/sec
10000
a
5000
0. 5000
I=
nIl
_
3000
w2
3500
]
4C100
o
3000
t/sec
3500
t/sec
Figure 6-55: Patient 6, Segment 3: Filtered Signals (L = 481)
L=481
M+(HR, CO) Both rose because of decreased depth of anesthesia.
AlM+
(HR, RPP)
M+(HR, SV)
M+(HR, VC)
M+(CO,RPP)
M+(CO,VC)
M+(RPP, VC)
M+(SV, CO)
M+(SV,RPP)
M+(SV, VC)
mult(HR,ABPM, RPP) (Correct)
mult(HR, ABPM, VC) (Spurious)
mult(HR,CVPM,RPP) (Spurious)
mult(HR, CVPM, VC) (Spurious)
127
4000
rnult(HR, SV, CO) (Correct)
128
,Fat|
I
W
11
-
a.
53
0
-;R
4
L
%3oo
l
3500
f
4000
3500
t/sec
4 IIIIAnn
100
I-r
50
_
C,,
0o
30 00
3500
500 I
n
30oo
4000
t/sec
3500
4000
/sec
0I X 104
1
-
JrI
o
4000
t/sec
0. 5
O-
3000
A
3500
3'00
40(20
t/sec
3500
4000
t/sec
4I nnnn
.. ..
.I.
Jl
a
aC 5000
2I
D n'
..v
I
I I=
3o00
3500
3000
40( 20
t/sec
Figure 6-56: Patient
6, Segment
3:
3500
t/sec
Filtered Signals (L = 601)
L=601
A+ (CO, RPP)
Both rose because of decreased depth of anesthesia.
Ml+(CO, VC)
ATM+(HR,CO)
M+(HR,RPP)
MI+(HR, SV)
M+(HR, VC)
M+(RPP, VC)
M+(SV, CO)
M+(SV, RPP)
M+(SV, VC)
mult(HR, ABPM, RPP) (Correct)
mult(HR, ABPM, VC) (Spurious)
mult(HR, CVPM, RPP) (Spurious)
mult(HR, CVPM, VC) (Spurious)
129
4000
rnult(HR, SV, C'O) (Correct)
130
6.2.4
Segment 4
The patient condition was steady. This period was uneventful.
200
10C
I
I
am
l-
> 100
50
0,
I
J
4000
4500
5000
4o00
,n
J
,
t/sec
A
I
4500
-. .
5000
rnn
·.
'
I
-4V00
Ix
5000
4500
/sec
/sec
105
J
0C. 0
.4
_c,
40oo
0 o or
- .r -
rlr
-. -w .-n
.
I
A
I
5000
I---r
I500
rr
t.~'~
·- · ··
vUUU
I 10o
nL
a- 1
,,,
t/sec
20CII
Z
A R
4500
4500
t/sec
5000
4oo
4500
5000
i/sec
x 1o04
I
W1~tZ
4000
4500
I-
5
1
w
0
A
VUoo
5000
4500
i/sec
i/sec
Figure 6-57: Patient 6, Segment 4: Original Signals
131
5000
60I
nI
IF
-
E
5
2C
4( I --~0boo
10TV
· [
·
Jt
I
l
-
4500
t/sec
5000
4000
---
1UUU
|
500
A
5000
4u00v
4000
I
4500
5000
t/sec
I
Iv
o
4500
t/sec
X 104
I
0
5000
t/sec
50 >1'
4000
4500
1
r
-
5
I'O.
n
u _
4000
x
rr
0-
mr
4500
t/sec
4000
5000
nn
III II
5000
4500
t/sec
5000
4500
t/sec
5000
J
V
-i1
w
a
I I.
40000
4500
t/sec
5000
4000
Figure 6-58: Patient 6, Segment 4: Filtered Signals (L = 61)
L=61
nmult(HR, ABP,
RPP) (Correct)
mult(HR, SV, CO) (Correct)
132
In
nJ
10
.1 X 0
Q- 40
m
L-
I'l
'4000
,..l
5
o
4500
5000
4'000
t/sec
5000
t/sec
1000
10 I I
JV
a
Lo 500
VIj
,I
·I
4500
'4.000
5000
4 00
4000
t/sec
x10
0o
1
0 0.5
5
nJJ J
4000
4500
5000
W
l_
-
4Vo00
t/sec
nnn
JJ JJ
5000
4
f
.J
4500
t/sec
lU
Er
a:
4500
4500
5000
t/sec
_
-
2
6000
A
~J
nn
JJ JJ
0
I.
4000
4500
t/sec
n
4000
5000
4500
t/sec
Figure 6-59: Patient 6, Segment 4: Filtered Signals (L = 121)
L=121
mult(HR, ABP.M, RPP) (Correct)
mult(HR, SV, CO) (Correct)
133
5000
nf,
~E
1
a
03 50
0
Ar!
oo00
4500
5000
5v
5
n
4v000
t/sec
j
OU
r70
70
4000
4500
5000
A,f~.
0
50 0
Ai---1
4500
4000
5000
t/sec
t/sec
4
x 1C0
I
5000
100
lI
c,\
I,,
UV
4500
t/sec
h'1
1
I I
0 !
Q
A
'L -L_~
·
v
4000
4500
-·
- i4 _
5000
4000
-boo
t/sec
anrar
_
III
II
AAn 4000
5000
4500
5000
2
~I
a 6000
4500
t/sec
U
4500
4000
5000
4000
t/sec
t/sec
Figure 6-60: Patient 6, Segment 4: Filtered Signals (L = 241)
L=241
invderiv(ABPM, RPP) (Spurious)
mnult(HR, SV, CO) (Correct)
134
55
-
2a
rn50
4
0
Ar
DO
401
Gu
5000
4500
t/sec
9
4000
5000
t/sec
1000
-
500
>
70
ni
40400
4500
5000
I
4600
t/sec
b
4500
4500
5000
/sec
x 104
m
1
_
0
Or
n_
-· 4
i
4vo00
4500
5000
_
4000
t/sec
----
cc
1.'rI
I
6000
Ann
·
n·
·
5000
t/sec
bUUU
L
4500
II-w
a
_
4000
4500
5000
t/sec
1
A
r,
400ooo
4500
t/sec
Figure 6-61: Patient 6, Segment 4: Filtered Signals (L = 361)
L=361
No constraints were obtained.
135
5000
6r
-1-1 f
Cn 50
m
o
73I
4[-
4500
t/sec
4o000
M .
-
f
|
400
50)00
4500
t/sec
5000
4500
tsec
5000
4500
t/sec
5000
4500
5000
1000
_
I:3 70
500O-
4500
4')00
tsec
50)00
4000
x 104
1
0
.
I!
4000
-·
-Iboo
.~~~~~~~~~~~~
4500
t/sec
__
5000
4000
brAA
I
4
a1
a 7000
ccN E
fiAnn
v0vv
4000
w
0
-
4500
t/sec
II
5000
_
"4boo
t/sec
Figure 6-62: Patient 6, Segment 4: Filtered Signals (L = 481)
L=481
M+(ABPM, SV) Both decreased overall.
M+(RPP, VC) (Spurious)
136
rr
50
0
> 4I
Ar
4500
t/sec
400
no
5000
400
4500
t/sec
5000
4500
5000
rIU
---
I VUV
·-
> 500
M70
an 4000
0
4500
t/sec
x 1C)04
0
A - -
4000
n
4'000
5000
>"'
"
4500
t/sec
t/sec
o
_
___________________________ _.
5000
4b00
4500
t/sec
5000
n 7000
nfAn
oouu
-
4000
4500
Au, r4 ---
4000
5000
-;
4500
t/sec
t/sec
Figure 6-63: Patient 6, Segment 4: Filtered Signals (L = 601)
L=601
M- (ABPM, CO) Both decreased overall.
AI (ABPM, SV) Both decreased overall.
M+ (SV, CO) Both decreased overall.
mult(HR, ABPM, RPP) (Correct)
mult(HR, SV, CO) (Correct)
137
5000
6.2.5
Segment 5
The patient experienced low ABP post bypass due to poor cardiac performance secondary
to a technically poor graft and possibly hypovolemia. Inotropic therapy (Dobutamine) was
given which potentially caused the patient to develop myocardial ischemia. Blood infusion
was performed to bring ABP back up.
100
uu
Il
60
n
,:C 1
--
> 50
s-JJ
1000
1500
0
10(D0
2000
~~~l~~~n~~.
t/sec
~
J
2000
-TU
r 100 .l I
Z
- II II
'~UUU
|
1500
2000
1000
1500
t/sec
t/sec
00
x 105
,
C)
0
.........
>
9 .1o000
L-L
1500
2000
1000
t/sec
'
G
1.
0-
Cr
x 104
'.*W.
r/
hI'I"f
-E
2000
. TT .-" " -.
1500
t/sec
20 00
1500
20 00
-j
r-
nI _
1.,,0
1000
I.
W-
nmnrrrr
(c
1000
2
2000
1500
t/sec
I-
31.5
·· ·
1500
1
1000
2000
t/sec
t/sec
Figure 6-64: Patient 6, Segment 5: Original Signals
138
10
50
--
a. 40
co
0
T-
U 5
A
.5{ _
I'l
1000
1 00
1500
2000
It
10oo0
t/sec
100
1000 I
rr 90
T
lrl
l
1500
2000
i'6oo
n x 104
l[
I
5
·-z
Ai
i'66
1000
0o .5
n
1500
2000
1000
~~n
III
1·
I
0a 8000
"1
II
vv00
I
1000
201 O0
'A
5 1.2
0
1500
t/sec
1500
t/sec
t/sec
a-
2000
4I-
11
5
1500
t/sec
t/sec
0o
·
> 500
1000
Iv
2000
t/sec
B
-
1500
2000
1
1000
A
A~~~~~
1500
t/sec
Figure 6-65: Patient 6, Segment 5: Filtered Signals (L = 61)
L=61
mnult(HR, ABPM, RPP) (Correct)
mult(HR, SV, CO) (Correct)
139
20100
50
10
a- 40
m
0
nn L
-
-
1000
|
1500
2000
5
t
n
1000oo
t/sec
1000
90
> 500
__
000
1000
2000
t/sec
100
IT
1500
orb
Y·
!
A\
I
1500
t/sec
U-o
1000
2000
1500
2000
t/sec
x 104
[ [
,,
0
1
r
5
o
> 0.5
n1__
1000
*1'
rs I
[
[
1500
2000
1000
t/sec
10000
.l
F-
f
vvv
1000
I
1.4
2000
|
.l
L 1.2
D
1000
1
-
1500
t/sec
2000
t/sec
aa- 8000
cc
-n---II
1500
[I
1500
t/sec
Figure 6-66: Patient 6, Segment 5: Filtered Signals (L = 121)
LJ=121
mult(HR, SV, CO) (Correct)
140
2000
Iou
lU
40
5
cn
1000
1500
t/sec
2000
>
A1
1o00o
1500
t/sec
2000
1500
2000
cnn~~~~~~~~~~~-.
DUU
nn
I'vv
9
90
an
v00oo
1500
2000
1oo00
t/sec
lU
t/sec
x 10 4
0 0.5
A5
7
n
100oo
1500
t/sec
2000
a
1500
t/sec
2000
1500
t/sec
2000
I1.L
I UUUU
a.
1o00o
8000
annn_
1000
1.2
Jw . J
0 .44
1500
t/sec
2000
i000
Figure 6-67: Patient 6, Segment 5: Filtered Signals (L = 241)
L=241
M + (ABPM, CO) Both dropped initially because of poor cardiac performance and hypovolemia, and started to rise following blood infusion.
M+(ABPM, SV) Both dropped initially because of poor cardiac performance and hypovolemia, and started to rise following blood infusion.
M+(SV, CO)
mult(HR, ABPM, RPP) (Correct)
mult(HR, SV, CO) (Correct)
141
50
- *
8
|
2
00 6
m 45
40*
1 0(30
1500
2000
1000
t/sec
r-· II
VVUU
I 95
C)
,_
1000
n
E
1500
_
_
1000
2000
t/sec
0 0.5
5
_
J
1500
t/sec
0
2000
10(00
4
[[
r
·
H. 1
H 1.2
-J
QU
_.
1000
I
1500
t/sec
1500
2C)00
t/sec
0_
Q 8000
mflnnn
2000
1
,
n1
1i000
1500
t/sec
x 10 4
[ I
It
..nnnn
I I [[II
2000
t/sec
100
cD
1500
2000
__
t
11
1000
1500
2C)00
t/sec
Figure 6-68: Patient 6, Segment 5: Filtered Signals (L = 361)
L=361
M+(ABPM,
CO() Both dropped initially because of poor cardiac performance and hypov-
olemia, and started to rise following blood infusion.
142
Q1
J'~lI
0(I 6
45
An
10400
A
1500
2000
1000
t/sec
2000
t/sec
50s )I
lUU I
I
1500
95
u,
9C600
1500
tsec
2000
A
1V00
1500
tsec
2000
x 10 4
.1
1
_
O
o 0.5
0
w4
i
_
nI __
i
1010o
1500
2000
1000
t/sec
---- ~
1.3
X 8000
I-U 1.2
0 11
7nfn
1500
2000
t/sec
YUUU
l10o 0o
1500
-
'iboo
2000
t/sec
1500
t/sec
Figure 6-69: Patient 6, Segment 5: Filtered Signals (L = 481)
L=481
No constraints were obtained.
143
2000
rn
n
oU
0
E 45 An
02
~~A
I
--
1000
1500
_
2000
_
1000
_
_
_
_
1500
_
2000
t/sec
t/sec
100
G
_
500
95
03
1000
1500
2000
1000
t/sec
1500
2000
t/sec
x104
O
O 0.5
n
>
A
_
_
1000
_
_
_
1500
t/sec
_
----\
2000
1000
1500
t/sec
2000
1500
t/sec
2000
nnn-.G
8000
7nAn
I uuu
5 1.2
-
01
W
--
1000
1500
t/sec
2000
1
, . I
1000
Figure 6-70: Patient 6, Segment 5: Filtered Signals (L = 601)
L=601
A/+ (SV, CO) Both dropped because of hypovolemia.
MA--(HR, CO) HR increased both as a compensatory response to decreasing CO due to
hypovolemia, and as a response to inotropic therapy.
A1--(HR, SV)
invderiv(SV,
CO) (Spurious)
mult(HR, ABPiM, RPP) (Correct)
mult(HR, SV, CO) (Correct)
144
6.2.6
Segment 6
ABP gradually rose as a result of switching to another inotrope (Adrenaline) and blood
infusion.
80
o
m 60
10
I
3000
2500
2ooo00
3000
200 VIII
L
Cn 100 0
I
A
2500
t/sec
2000
5
2500
t/sec
50CIvf-
"1 II
u2000
I
11
III
t/sec
0
11
8
0
ArI
-200o
I11
1,10111.
11,II''
00
2000
3000
'MMM1M1,p4pWiJU_,;
1111 11
HIM
2500
3000
t/sec
x 1C5
..
0
,
0
_
1n
2000
2500
t/sec
2500
3000
3000
t/sec
x 104
5_
, O1E
a.
a.
2
n'
D1
-EI''
2000
2500
3000
r.E,_
2000
t/sec
2500
t/sec
Figure 6-71: Patient 6, Segment 6: Original Signals
145
3000
8
TV!
I.!
6 _
O_
°
60
Ans
.
2000oo
2500
3000
2500
t/sec
3000
t/sec
In-I UUU
III
I--
I 95
)> 500
nI __
2500
/sec
R2 oo
3000
2o00
2500
3000
t/sec
n x 104
Iv
00
01
5
I _
n1
(l
2ooo00
rx
1. -1.
2500
t/sec
3000
2%00
2500
3000
t/sec
104
- 1.6
.
_
aL
a-
CE
1.4
1
nr
_
2000
uJ
2500
1
_
'2'00
3000
t/sec
2500
t/sec
Figure 6-72: Patient 6, Segment 6: Filtered Signals (L = 61)
L=61
mult(HR, SV, CO) (Correct)
146
3000
n
OU
a6
50
m
co
At
A
2500
2boo
200
3000
t/sec
10
fnnn
I UUU
I
M 95
> 500
uE
vll
I
2500
N2 oo
3000
2000oo
10
,x
2500
3000
2500
3000
tsec
t/sec
4
3000
t/sec
I
fV
2500
4
IJ
0
5
0
1
II
2'000
2500
_
2o00
3000
t/sec
1.2
a.
a.
t/sec
x 104
4
-
' 1.4
w
1
W.
0.8
-
2000
LU I
2500
t/sec
_
'200
3000
2500
t/sec
Figure 6-73: Patient 6, Segment 6: Filtered Signals (L = 121)
L=121
mult(HR,ABPM, RPP) (Correct)
mult(HR, SV, CO) (Correct)
147
3000
8
IL 50
m
6n
O_
o6
2
dn
2500
20oo
3000
t/sec
4
3000
2500
3000
I---n
I UUU
nf
IIB
.vv
CT
I 95
> 500
n1
200oo
7
2500
t/sec
1\
_
..
2500
3000
2o00
t/sec
t/sec
4
x 10
11
00
AII
f.
0
5
I
1
rI
2oo
2500
3000
200oo
t/sec
.2
aa-
x 104
I
w
1.6
1.4
0 .I
n a
I
2000
2500
3000
t/sec
1
Ir
2500
3000
t/sec
v4
-
20(30
2500
t/sec
Figure 6-74: Patient 6, Segment 6: Filtered Signals (L = 241)
L=241
mult(HR,ABPM, RPP) (Correct)
148
3000
60
a
co 50
2 6-
_
An
200ooo
-
o
-
A I
Jl
z
2500
t/sec
3000
2000
1000
95
> 500
nn
10
o
3000
2500
t/sec
3000
2000
2500
3000
t/sec
5
I
n
_
I
2000
x 10o
-1
·
3000
·
i 1.4
1
_ _1_
n
U.o0
2500
t/sec
1 .z
cc
|
I |
i-L
2500
t/sec
x 104
n
2000
aa-
[
rI
__
2000
3000
t/sec
100
YI
2500
w
2000
-
0
s
2500
1
F
_
200
3000
t/sec
2500
t/sec
Figure 6-75: Patient 6, Segment 6: Filtered Signals (L = 361)
L=361
M+(SV, CO) Both rose after blood infusion.
deriv(SV, CO) (Spurious)
rmult(HR, SV, CO) (Correct)
149
3000
n,
Du
r
Tc
"7
-
a
50
6
0
n4F
-
2500
20 00
2600
3000
t/sec
14I*nfr
I VUU
I 95
> 500
on
I!
)00
0
2500
I
5
_-
In
_
lU
3000
!
2'o00
t/sec
1
2500
n
20ooo
3000
'oo
2500
3000
t/sec
X 104
I- . ·I
I- 1.4
.U
1
na
3000
Vsec
t/sec
aa:
2500
4
200
1. 11J_
3000
t/sec
100
,x10
2500
uJ
w
0
2500
t/sec
14
e
l-
2000
2000
3000
2500
t/sec
Figure 6-76: Patient 6, Segment 6: Filtered Signals (L = 481)
L=481
M+(SV, CO) Both rose following blood infusion.
deriv(SV, CO) (Spurious)
mult(HR,ABPM, RPP) (Correct)
mult(HR, ABPM, VC) (Spurious)
150
3000
-- %1-
UV
50
0 r,r
An
Y000
2500
t/sec
3000
2o00
1 uuu
IUU
2500
t/sec
3000
2500
3000
l-
> 500
95
on
- l
A
!
$
2-000
2500
3000
2'000
Vsec
X 10
Vsec
4
IV
0 Ai
A
n
2'000
2500
3000
2'000
t/sec
1.2
x104
3000
1.6
a1
w
0.800
2000
2500
t/sec
2500
1.4
1.2
3000
t/sec
t/sec
Figure 6-77: Patient 6, Segment 6: Filtered Signals (L = 601)
L=601
M-(HR,
AT) HR decreased following blood infusion. Lagging effect of vasoconstriction
caused AT to increase.
M- (HR, SV) HR decreased and SV increased following blood infusion.
M+(SV, AT)
deriv(ABPM, RPP) (Spurious)
deriv(ABPM, VC) (Spurious)
deriv(SV, CO) (Spurious)
mult(HR, ABPM, RPP) (Correct)
mult(HR, ABPM, VC) (Spurious)
mult(HR, CVPM, VC) (Spurious)
mult(HR, SV, CO) (Correct)
151
Chapter 7
Discussion
The goal of this thesis is to develop a system for learning qualitative models from physiological signals. In Chapter 1 we mentioned two potential applications for such a system.
First, the system could be a useful tool for the knowledge acquisition task of inducing useful models from vast amounts of data. Second, the system could be incorporated into an
intelligent patient monitoring system to perform adaptive model construction for diagnosis
in a dynamic environment. In this chapter, we evaluate the performance of the system in
knowledge acquisition and identify sources of error. We then examine its applicability in
diagnostic patient monitoring.
7.1
Validity of Models Learned
The results in Chapter 6 show that reasonable qualitative models can be learned from raw
clinical data. Model constraints in our "gold standard" model constructed in Section 4.2
and other useful constraints showed up repeatedly in the models learned from our clinical
data. These include:
* constraints valid in general such as mult(HR, SV, CO) and mult(HR, ABPM, RPP).
* constraints valid in specific patient conditions, possibly representing compensatory
mechanisms, such as M- (HR, CO) and M- (CO, AT) in hypovolemia.
* constraints valid under the effect of certain drugs. For example, M+ (SV, CO) showed
up in patients on beta-blockers because of their steady heart rate, and M+ (ABPM, AT)
showed up in patients with an increased dosage of GTN causing vasodilation.
152
7.1.1
Model Variation Across Time
As discussed in Chapter 3, GENMODEL learns a qualitative model by creating an initial
search space of all possible QSIM constraints, and successively pruning inconsistent con-
straints upon each given system state. Therefore if the system changes within the modeling
period (in our case 16.7 minutes) resulting in a different underlying model, neither the old
model nor the new model may be obtained. Constraints in the old model are pruned be-
cause they are inconsistent with the states after the system change. Constraints in the new
model are pruned before the system change because they are inconsistent with the previous
system. This may explain cases when we obtain very few or no model constraints.
For
example, if a patient is previously stable with an increasing relationship between the heart
rate (HR) and the cardiac output (CO):
M+(HR, CO)
but develops hypovolemia in the middle of a modeling process, resulting in a decreasing
cardiac output and a compensatory mechanism involvingan increasing heart rate, the new
valid constraint is:
M-(HR, CO)
But this will not appear in the final model because at the onset of hypovolemia, this constraint has already been pruned by GENMODEL according to states corresponding to the
previously stable condition. Furthermore, the previously valid constraint M+(HR, CO)
will be pruned because it is now inconsistent with the system states corresponding to hypovolemia.
7.1.2
Model Variation Across Different Levels of Temporal Abstraction
The models learned in Chapter 6 varied across different levels of temporal abstraction, represented by the filter length L. For example, constraints which involve the skin-to-core
temperature gradient AT representing the level of vasoconstriction in the body, generally
appeared only under large values of L, i.e. in coarser time scales. This means the response of AT generally lags behind the responses of other parameters.
This may be due
to the considerable heat capacity of the body causing a delay in the measurable effects of
153
vasoconstriction.
In general, we observe that fewer model constraints were learned with decreasing L or
finer time scales. This can be due to the following reasons:
* As discussed in Section 5.2.4, smaller values of L and therefore smaller values of a
correspond to larger cutoff frequencies in the lowpass Gaussian filters, and larger band-
widths in the bandpass filtering operation equivalent to the cascade of the Gaussian
filter with the differentiator. This reduces the amount of noise rejection achieved, and
results in noise sensitivity problems in detecting zero crossing points and therefore
less accurate segmentation. This additional amount of noise may have caused correct
constraints to be pruned, resulting in fewer or even no constraints left in the final
model.
* Smaller values of L correspond to faster processes which may have more dynamic
models. As discussed in Section 7.1.1, a system change within a modeling period can
cause constraints belonging to both the previous and the current model to be pruned,
resulting in a smaller model or even one with no constraints.
7.1.3
Model Variation Across Different Levels of Fault Tolerance
We observe that in general the size of the model learned increases with increasing levels of
fault tolerance. A fault tolerance level of q7means that GENMODEL allows for inconsistent
states up to a fraction
a constraint.
of the total number of states in the system behavior before pruning
Therefore with larger 7, fewer constraints will be pruned and the resulting
model will contain more constraints.
An indication of r7being set too high is that conflicting constraints start to appear. For
example, in Patient 5 with L = 61 (Figure 6-30), both
M+(CVPM, AT)
and
M-(CVPM, AT)
appear in the model learned. This is because both CVPM and AT are relatively steady
and contain only few inc and dec segments which distinguish between the M+ and M154
constraints. Within a high level of tolerance, the distinction is obscured.
7.1.4
Sources of Error
False Positives
In the models learned, we observe that spurious constraints sometimes appeared in the
resulting model. For example, in Patient 1 (L = 601), we obtained the spurious constraint:
inv.deriv(ABPM,RPP)
This can be due to several possible reasons:
* The waveforms are relatively smooth with few critical points. This results in a system
behavior with few states, corresponding to few examples for learning.
Now it is
relatively probable that these examples are consistent with the incorrect constraint.
For instance, if whenever ABPM decreases, RPP is positive, then the above incorrect
invderiv
constraint will be learned.
* The level of fault tolerance is set too high resulting in incorrect constraints not being
pruned.
False Negatives
We observe that even constraints that are generally valid in all conditions, such as
mult(HR, SV, CO)
did not appear in every model learned. There are several possible reasons for this:
* Since few states are available in the data segment resulting in few examples for learning, if these examples are corrupted by noise, the correct constraint will be pruned.
* Values corrupted by noise are recorded as corresponding values by the system. This
problem is explained further in Section 8.1.1.
* The level of fault tolerance is set too low resulting in correct constraints being pruned.
155
Landmark Values
Temporal abstraction refers to how close two times have to be before we label them as the
same distinguished time point. Similarly we have to decide how close two function values
have to be before we label them as the same landmark value. If the tolerance is set too low,
we may amplify trends of relatively steady signals. This is the case in the heart rate signals
of Patients 4 and 5 (Figures 6-23 and 6-30) which are relatively steady due to the effect of
beta-blockers. The fluctuations within 2-3 beats per minute are amplified into a series of
inc (increasing) and dec (decreasing) segments. The whole segment might well have been
labeled as std (steady) if we had set the tolerance appropriately.
7.2
Applicability in Diagnostic Patient Monitoring
From the models shown in Chapter 6, we see that constraints of models learned do track
changes in patient condition over time. For example, the following changes were tracked:
Compensatory mechanisms during shock e.g. the constraints M-(HR, CO) and
M- (CO, AT) learned when the patient experienced hypovolemia.
Effects of drugs e.g. the constraint M+ (SV, CO) tracked the effect of beta-blockers because of the patient's relatively constant heart rate, and the constraint M+ (ABPM, AT)
tracked the effect of an increased dosage of GTN causing vasodilation.
7.2.1
A Learning-Based Approach to Diagnostic Patient Monitoring
Since model constraints learned track patient condition over time, we might be able to
build a diagnostic patient monitoring system based on our learning system. The patient
monitoring system continually learns models from patient data and detects changes in the
models learned. Diagnoses are made based on these changes. This learning-based approach
to diagnostic patient monitoring is summarized in Figure 7-1.
The traditional history-based approach to diagnostic patient monitoring goes in the
opposite direction.
It generates histories based on different models. These histories are
matched with the patient data. Diagnoses are based on models corresponding to histories
that best match the patient data. This approach can be achieved by a hypothesize-testrefine cycle as shown in Figure 7-1 [6].
156
Learning-based
History-based
Approach:
Approach:
Diagnosis
Refine
Figure 7-1: Two approaches to diagnostic patient monitoring. In the learning-based approach, models are continually learned from the patient data. In the history-based approach,
a hypothesize-test-refine cycle is used to generate models that best match the patient data.
In each approach, diagnoses are made based on the current model.
The learning-based approach may be more efficient since the hypothesis model is generated directly from the patient data and there is no need for a hypothesize-test-refine
cycle.
7.2.2
Generating Diagnoses Based on Models Learned
We need to be careful in making diagnoses based on models learned. The same model
constraint can correspond to different diagnoses in different contexts. For example,
* The constraint M + (HR, CO) can correspond to a healthy person performing physical
exercise, when the rise in heart rate increases the cardiac output. It can also correspond to a hypovolemic condition when the compensatory effects of increased heart
rate, increased myocardial contractility and vasoconstriction successfully increase the
cardiac output, but the patient is still in hypovolemia.
* The constraint M- (HR, CO) can correspond to a person in hypovolemic shock when
the increasing heart rate is incapable of compensating for the decreasing cardiac output. The same constraint can also be obtained when blood infusion is performed in
response to the hypovolemia. In this case, the cardiac output will increase because of
157
the blood infusion, and the heart rate will decrease to normal.
Therefore different patient conditions may result in the same model constraint. However, this may not be a problem for applying the learning approach to diagnostic patient
monitoring for the following reasons:
* Most changes in patient condition will involve changes in many parameters and in
multiple constraints.
* If only few parameters are monitored, a semi-quantitative representation may be used.
This may allow more fine grained distinctions between patient conditions.
158
Chapter 8
Conclusion and Future Work
This thesis describes work in learning qualitative models from clinical data corrupted with
noise and artifacts. The learning system consists of three parts:
Front-end Processing removes artifacts and smooths the signals according to the level
of temporal abstraction desired.
Segmenter segments the signals at critical points producing a qualitative behavior of the
system.
GENMODEL
learns a qualitative model from the qualitative behavior.
We tested the system on clinical data obtained from six patients during cardiac bypass
surgery. Useful model constraints were obtained, representing the following categories of
information:
General Physiological Knowledge e.g. mult(HR, SV, CO), mult(HR, ABPM, RPP).
Compensatory Mechanisms During Shock e.g. M-(HR, CO) and M-(CO, AT) representing the mechanisms of tachycardia and vasoconstriction to compensate for a
hypovolemic shock.
Effects of Drugs e.g. M+(SV, CO) representing the effect of beta-blockers producing a
steady heart rate, and M+(ABPM, AT) representing the effect of vasodilators such
as GTN causing vasodilation which decreases both the arterial blood pressure and the
skin-to-core temperature gradient.
159
The learning system might be used in a diagnostic patient monitoring system to learn
models from patient data. Based on these models, diagnoses of the patient condition can
be made. This provides a learning-based approach to diagnostic patient monitoring, which
is different from the traditional history-based approach. The learning-based approach may
be more efficient because it avoids the hypothesize-test-refine cycle.
8.1
Future Work
Promising directions for future work include:
Front-end Processing
* Investigate wavelet transforms for multiresolution signal analysis in achieving
different levels of temporal abstraction in the resulting qualitative behavior [35].
GENMODEL
* Investigate more robust ways of dealing with data corrupted by artifacts, e.g.
examine the applicability of results in PAC learning from data corrupted with
attribute noise.
* Investigate methods of using corresponding value information in noisy data. (See
Section 8.1.1.)
Patient Monitoring
* Investigate more precisely the relationship between levels of temporal abstraction
and delays in physiological responses. For example, the system can be tested
in the domain of pharmacokinetics to relate the level of temporal abstraction
at which appropriate constraints are learned to the onset of action of different
drugs.
* Investigate the context information necessary for accurate diagnoses based on
learned models.
8.1.1
Using Corresponding Values in Noisy Learning Data
In Section 3.4.4 we mentioned that since we are learning from noisy signals, we have to
allow for errors in the qualitative state history produced from the signals by the front-end
160
processor and the segmenter.
We accommodated this noise in the qualitative behavior
by introducing fault tolerance into GENMODEL. Specifically, we set a noise level r7 to a
fraction of the total number of qualitative states, such that a constraint is not pruned until
it has failed for this many states.
The noisy learning data introduce another difficulty in GENMODEL - that of locating
corresponding values. When two or more functions reach landmark values in the same
qualitative state, these landmark values are noted to be corresponding values. However,
if the learning data is noisy, we do not know which states are valid and which are not. If
we continue to label all landmark values which coexist in the same state as corresponding
values, we will come up with a number of incorrect corresponding value sets. These incorrect
sets will consistently cause constraints that check for corresponding values (i.e. M + , M-,
add, mult) to fail and ultimately be pruned, even if they are valid constraints. This is in
fact the approach currently taken in our learning system, and can be regarded as a source
of error.
One simple solution to this problem is to give up corresponding value checking and simply rely on direction-of-change consistency for checking monotonic constraints.
Without
the magnitude information provided by the corresponding values, a certain level of performance can still be achieved, as in attempts of Bratko et al [4] and Varsek [38] in learning
the U-tube model. However, omitting corresponding value checking results in much weaker
forms of qualitative constraints, which no longer correspond to Kuipers' original definitions
in [20]. For example, without corresponding values, the monotonic constraints M + and
.A1- no longer require a one-to-one mapping between values of their function arguments, as
they do before (described in Section 2.1). Now if we have M + (a, b), if a increases steeply
to the same value a(1l) in two different states, b can increase steeply to a large value b(l) in
one state, and increase only slightly to a small value b(2) in the other state, as long as it
increases at all. Magnitudes no longer need to correspond. (Figure 8-1)
Using landmark intervals to represent corresponding value information in noisy
learning data
In the previous section we mentioned that exact corresponding values may be difficult to
obtain from noisy learning data because we do not know which states are valid and which are
not. Here we propose using landmark value intervals together with landmark values to allow
161
a(1
ne
I
b(1
b(2
t(O)
t(1l)
t(2)
t(3)
t(4)
Time
Figure 8-1: The two functions a and b shown obey direction-of-change consistency for the
qualitative constraint M+(a, b), but not magnitude consistency.
for an error tolerance in the corresponding values obtained. We show that this is analogous
to using a boundingenvelopeto represent a monotonic function in semi-quantitative methods
[22, 16].
Error tolerance in corresponding values can be achieved by allowing a point to cor-
respond to a region which represents an error band within which the true corresponding
landmark value may exist. A landmark value a(ti) corresponds to a closed landmark value
interval [b(t2 ), b(t3 )] if and only if there exists a corresponding pair between the landmark
value a(ti) and a value within the closed interval [b(t2 ), b(t 3)].
Furthermore, we assume that the noise in the learning data is of a reasonable magnitude,
such that a value can be mislabelled by a range of at most one landmark value. Therefore,
a landmark value interval can extend by at most two landmark values (one landmark value
greater than and one less than the true value).
Searching for corresponding sets is similar to before. We proceed down the qualitative
state history, looking for landmark values reached in the same state.
But now, instead
of simply recording each set of values, we check first to see if one of the corresponding
values already exists within a corresponding set. If this is the case, and if the other new
corresponding value is adjacent to the existing corresponding value in the landmark list,
then we extend the existing value into an interval to include the new value. However, if the
162
new corresponding value differs from the existing corresponding value by more than one
landmark value, we can conclude that a one-to-one mapping does not exist between the two
functions. Therefore, we can prune all monotonic constraints (M+ and M-) between the
two functions, and form a new set of corresponding values for constraint checking with add
and mult, since add and mult do not require a one-to-one mapping between values of its
argument functions.
For example, if we have corresponding values (pl, qi), and we come across the state
QS(p,t3) = <p, std >
QS(q,t3) = < q2, std >
Then if q and q2 are adjacent to each other in the landmark list, then we have the new
corresponding pair
(P1, [ql, q2])
assuming q < q2.
However, if ql and q2 are not adjacent to each other in the landmark list, then we can
prune the followingconstraints
M+ (p, q)
M- (p, q)
and form the new corresponding value set
(pl, q2, .. )
for constraint checking with add and mult.
New constraint rules can be added to accommodate intervals in corresponding pairs.
For example, a rule similar to Kuipers' Proposition B.1 in [20] can be added as follows:
Suppose M + (f, g), with corresponding values (p, [ql, q2]), and
QS(f, t1 , t2 ) = < (p,p'), dec >,
QS(g, t1 , t 2 ) = < (q, q'), dec >,
where q E [ql, q2]
Then one of the following two possibilities must be true at t 2:
(1)
f(t 2 ) =p, g(t2) E [ql, q2];
(2) f(t2) > p, g(t2) > q1.
163
b(t)
estimated function
upper envelope
-
boundary
/
lower envelope
,
boundary
b(l).
b(O)
----a(O)
a(t)
Corresponding value pair:
(a(O),[b(O),b(1)])
Figure 8-2: Incorporating intervals into corresponding value sets is analogous to adding a
bounding envelope to monotonic functions.
Incorporating intervals into corresponding values is analogous to bounding monotonic
functions in semiquantitative methods [22, 16]. The bounding envelope represents a region
which bounds all real behaviors of the given system with a certain probability p. Therefore
if we have M+(a, b), i.e. a = f(b) where f(x) is a monotonically increasing function, then if
we know at t(O) a is at a(O), we can be reasonably sure (with confidence p) that b lies within
the envelope of f(a(O)). This is analogous to the corresponding value pair (a(O), [b(O),b(l)])
where [b(O),b(l)] represents the envelope of f(a(O)) (Figure 8-2).
164
Bibliography
[1] J. Babaud, A.P. Witkin, M. Baudin, and R.O. Duda.
Uniqueness of the Gaussian
kernel for scale-space filtering. IEEE Transactions on Pattern Analysis and Machine
Intelligence, 8(1):26-33, January 1986.
[2] G. Balestra and D. Liberati. Qualitative simulation of urea extraction during dialysis.
IEEE Engineering in Medicine and Biology, 11:80-84, June 1992.
[3] A. Blumer, A. Ehrenfeucht, D. Haussler, and M.K. Warmuth. Occam's razor. Infor-
mation Processing Letters, 24(6):377-380,April 1987.
[4] I. Bratko, S. Muggleton, and A. Varek.
Learning qualitative models of dynamic sys-
tems. In Proceedings of the International Workshop on Inductive Logic Programming,
pages 207-224, 1991.
[5] E.W. Coiera. Generating qualitative models from example behaviours. DCS Report
8901, Department of Computer Science, University of New South Wales, Sydney, Australia, May 1989.
[6] E.W. Coiera. Reasoning with qualitative disease histories for diagnostic patient monitoring. PhD thesis, School of Electrical Engineering and Computer Science, University
of New South Wales, 1989.
[7] E.W. Coiera.
The qualitative representation of physical systems.
The Knowledge
Engineering Review, 7(1):55-77, 1992.
[8] B.C. Falkenhainer and R.S. Michalski. Integrating quantitative and qualitative discovery: The ABACUS system. Machine Learning, 1:367-401, 1986.
165
[9] F.L. Gobel, L.A. Nordstrom, R.R. Nelson, C.R. Jorgensen, and Y. Wang. Rate-pressure
product as an index of myocardial oxygen consumption during exercise in patients with
angina pectoris. Circulation, 57:549-556, 1978.
[10] I. Gratz, J. Kraidin, A. Jacobi, N.G. deCastro, P. Spagna, and G.E. Larijani. Continuous noninvasive cardiac output as estimated from the pulse contour curve. Journal
of Clinical Monitoring, 8(1):20-27, January 1992.
[11] A.C. Guyton.
Textbook of Medical Physiology.
Saunders, Philadelphia,
PA, sixth
edition, 1981.
[12] D.T. Hau. A waveform shape recognition system based on a blackboard architecture.
Bachelor's thesis, Department of Electrical Engineering and Computer Science, MIT,
June 1992.
[13] D.T. Hau and E.W. Coiera. Learning qualitative models from physiological signals. In
Proceedingsof the AAAI Spring Symposium Series: Artificial Intelligence in Medicine,
pages 67-71, Stanford, CA, 1994.
[14] L. Ironi, M. Stefanelli, and G. Lazola. Qualitative models in medical diagnosis. In
E. Keravnou, editor, Deep Models for Medical Knowledge Engineering. Elsevier, Amsterdam, The Netherlands, 1992.
[:15] J.R.C. Jansen, K.H. Wesseling, J.J. Settels, and J.J. Schreuder. Continuous cardiac
output monitoring by pulse contour during cardiac surgery. European Heart Journal,
11(Supplement I):26-32, 1990.
[16] H. Kay and L.H. Ungar. Deriving monotonic function envelopes from observations.
In Proceedings of the Seventh International Workshop on Qualitative Reasoning about
Physical Systems, pages 117-123, 1993.
[:17] Michael J. Kearns and Umesh V. Vazirani. Topics in computational learning theory.
Preliminary draft.
[18] G. Kendon.
An investigation of back-propagation for arterial blood pressure wave
classification. Master's thesis, Department of Artificial Intelligence, University of Edinburgh, September 1992.
166
[19] B. Kuipers. Qualitative simulation in medical physiology: A progress report. Technical
Report MIT/LCS/TM-280,
Laboratory for Computer Science, MIT, Cambridge, MA,
June 1985.
[20] B. Kuipers. Qualitative simulation. Artificial Intelligence, 29:289-338, 1986.
[21] B. Kuipers. Qualitative simulation as causal explanation. IEEE Transactions on Sys-
tems, Man, and Cybernetics, 17(3):432-444,May/June 1987.
[22] B. Kuipers and D. Berleant. Using incomplete quantitative knowledge in qualitative
reasoning. In Proceedings of the Seventh National Conference on Artificial Intelligence,
pages 324-329, 1988.
[23] D. Marr and E. Hildreth. Theory of edge detection. Proc. Roy. Soc. London, 207:187217, 1980.
[24] T.M. Mitchell. Version spaces: A candidate elimination approach to rule learning. In
Proceedingsof the Fifth International Joint Conference on Artificial Intelligence,pages
305-310, Cambridge, MA, 1977.
[25] T.E. Oh, editor. Intensive Care Manual. Butterworth, Sydney, Australia, third edition,
1990.
[26] A.V. Oppenheim and R.W. Schafer. Discrete-time Signal Processing. Prentice Hall,
Englewood Cliffs, NJ, 1989.
[27] G.D. Plotkin.
Automatic Methods of Inductive Inference. PhD thesis, University of
Edinburgh, August 1971.
[28] B.L. Richards, I. Kraan, and B.J. Kuipers. Automatic abduction of qualitative models.
In Proceedings of the Tenth National Conference on Artificial Intelligence, pages 723728, 1992.
[29] J. Rissanen. Modeling by shortest data description. Automatica, 14:465-471, 1978.
[30] R. L. Rivest. Learning decision lists. Machine Learning, 2(3):229-246, 1987.
[31] L.J. Saidman and N.T. Smith, editors. Monitoring in Anesthesia. Butterworth, Boston,
MA, second edition, 1984.
167
[32] R.C. Schlant and R.W. Alexander, editors.
Hurst's the heart: arteries and veins.
McGraw-Hill, New York, 8th edition, 1994.
[33] W.M. Siebert. Circuits, Signals, and Systems. The MIT Press, Cambridge, MA, 1986.
[34] M. Specht, C. Wichmann, C. Artenburg, B. Kuss, and K. Reinhart.
The influence
of vasoactive drugs on continuous cardiac output measurement by the pulse contour
method. Critical Care Medicine, 19(4):S24, April 1991.
[35] G. Strang.
Wavelets and dilation equations:
a brief introduction.
SIAM Review,
31(4):614-627, December 1989.
[36] G.A. Tannenbaum, D. Mathews, and C. Weissman. Pulse contour cardiac output in
surgical intensive care unit patients. Journal of Clinical Anesthesia, 5(6):471-478,
November/December 1993.
[37] L.G. Valiant. A theory of the learnable. Communications of the ACM, 27(11):11341142, November
1984.
[38] A. Varsek. Qualitative model evolution. In Proceedings of the Twelfth International
Joint Conference on Artificial Intelligence, pages 1311-1316, Sydney, Australia, August
1991.
[39] C. Weissman, E.J. Ornstein, and W.L. Young. Arterial pulse contour analysis trending
of cardiac output: hemodynamic manupulations during cerebral arteriovenous malfor-
mation resection. Journal of ClinicalMonitoring, 9(5):347-353, November 1993.
[40] K.H. Wesseling, B. deWit, J.A.P. Weber, and N.T. Smith. A simple device for the
continuous measurement of cardiac output.
Advances in Cardiovascular Physiology,
5:16-52, 1983.
[41] P.L. Wilkinson, J.V. Tyberg, J.R. Moyers, and A.E. White.
Correlates of myocar-
dial oxygen consumption when afterload changes during halothane anesthesia in dogs.
Anesthesia and Analgesia, 59:233-239, 1980.
[42] J.B. Wyngaarden, L.H. Smith, and J.C. Bennett, editors. Cecil Textbook of Medicine.
Saunders, Philadelphia, PA, 19th edition, 1992.
168
[43] A.L. Yuille and T.A. Poggio. Scaling theorems for zero crossings. IEEE Transactions
on Pattern Analysis and Machine Intelligence, 8(1):15-25, January 1986.
169