Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
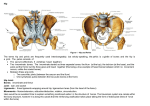
Unit VI – The Hip Objectives: At the completion of this unit the student will be able to: 1. 2. 3. 4. Identify the primary bony landmarks of the hip joint and upper leg. Identify the articulations that form the hip joint. Identify the key ligamentous and capsular structures of the hip joint. Discuss the importance of the ligaments and capsule to the stability of the hip joint. 5. Name the motions of the hip joint and primary muscles that perform these motions and their locations. 6. Discuss the relationship between the hip joint and the pelvis above, and the knee below. 7. Apply anatomy knowledge of this area to relevant issues for the dancer. Bony Structures of the Hip Joint and Upper Leg The bony components of the hip joint include the acetabulum that is part of the pelvis discussed in the previous unit. The lower portion of the pelvis makes up the proximal portion of the hip joint. The distal portion of the hip joint articulation is located on the femur bone. The femur extends to the knee joint as well, so these articulations are intimately related as they form the lower body kinetic chain. The Acetabulum The acetabulum is deep socket formed by the junction of the ilium, the pubis, and the ischium of the pelvis. It is located on the lateral aspect of the pelvis and forms a bowl-like shape where the head of the femur articulates. There is a horseshoe shaped articular cartilage that lines the top side of the acetabulum. The lower portion is called the acetabular notch and does not come in direct contact with the femoral head. The Femur Bone The femur is the longest and heaviest bone in the human body. The femoral head at its superior end is a smooth, spherical surface that articulates with the acetabulum to form the hip joint socket. The femoral head is covered with articular cartilage except at the fovea or tip where a small area for the ligamentum teres attachment is located. The ligamentum teres connects the femoral head to the acetabular notch. Another important landmark on the femur is the femoral neck. It is the area just distal to the femoral head where the bone constricts in. This is a frequent site of fracture in the elderly. Just distal to the femoral neck is the greater trochanter and the less trochanter. These are rough, bony projections that serve as muscle attachment sites that will be discussed below. The shaft of the femur is the long middle section and is roughly a triangular shape. At the distal end of the femur are the lateral and medical condyles. These are smooth articular surfaces that make up the proximal portion of the knee joint below. On the posterior portion of the femur shaft is the linea aspera. It is a prominent double ridge to which the adductor and vastus muscles attach. Between the two distal condyles, on the posterior aspect of the distal femur is a large opening called the intercondylar fossa. Variations in Hip Joint Angles Among Individuals The angle of the pelvis under the spine places the acetabulum of the hip joint in an anterior and inferior position. At the same time, the femoral head is angled obliquely medially, superiorly, and anteriorly in relationship to the shaft of the bone below. The angular relationship of the acetabulum and the femoral head varies among individuals. The average angle between the shaft of the femur and the femoral neck is 135 degrees. The anterior orientation of the neck of the femur to the acetabulum is normally 10-30 degrees. This is called anteversion and if the anteversion angle is small the ball portion of the femur fits well into the acetabulum and the joint will have good hip external rotation. If, however, the anteversion angle is large the anterior part of the femoral head is more exposed and can lose contact with the acetabulum and the lateral rotation of the hip joint will be reduced. These anatomical variations in bones and in joint articulations can determine available range of motion at a joint. This can be an issue for a dancer if anteversion in the hip reduces hip external rotation. This is a bony configuration that cannot be changed or stretched to increase. Ligament and Capsular Structures of the Hip There are several important structures that provide additional stability to the hip joint. The labrum is the fibrocartilaginous ring that attaches to the rim of the acetabulum. It is like a rubber washer ring that encircles the opening of the acetabulum and helps to increase the depth of the hip socket and hold the femoral head in place. The capsule of the hip attaches all the way around the rim of the acetabulum and down to the base of the neck of the femur. It is thick and reinforced by ligaments. The primary ligaments on the anterior of the hip joint are the iliofemoral ligament and the pubofemoral ligament. The iliofemoral ligament is shaped like a V and is the stronger of the two ligaments. It passes from the anterior inferior iliac spine down onto the line separating the femoral neck from the lesser and greater trochanters. The pubofemoral ligament runs from the pubic region of the pelvis to area just above the lesser trochanter on the femur. When viewed schematically these ligaments make a “Z” across the front of the hip capsule. These ligaments serve as “check rings” for the motions at the hip. A portion of the “Z” ligament is taut with flexion or extension of the hip, while other portions are taut during abduction and abduction. All portions of the “Z” ligament are taut with external rotation of the hip. These ligaments serve to increase joint stability and help protect the joint from injury when moving in extreme motion positions. The capsule helps deepen the hip joint space, as well as forming a fibrous ring around the hip joint area. The additional ligament structures further protect the stability of the joint. Movements of the Hip There are many motion options at the hip joint. Motion can occur with the pelvis fixed and the femur below moving, or the femur can be fixed and the pelvis can move from above. When the pelvis is fixed the femur motion includes: Hip Flexion – this occurs when the angle between the anterior surface of the thigh and the trunk decreases; bringing the knee to the chest is hip flexion. There is greater range of motion for hip flexion when the knee is bent. If the knee is straight the flexibility of the hamstring limits the motion of the leg toward the chest. Hip Extension - this occurs when the angle between the posterior surface of the thigh and the trunk decreases. This is taking the leg to the back . There is much less available range of motion into hip extension compared to hip flexion. A dancer can appear to have more hip extension by increasing lumbar lordosis in the trunk. Rocking the pelvis forward over the femur can also give the illusion of hip extension. When the knee is bent hip extension is reduced due to muscle length limitations for the quadriceps muscle in the front of the upper leg. Hip Adduction – this occurs when the thigh moves toward midline of the body or past midline to cross in front of the other leg Hip Abduction – this occurs when the thigh moves away from the middle of the body. When the femur is in neutral rotation there is only about 40 degrees of hip abduction because the leg makes contact between the femoral neck and the upper edge of the acetabulum. More abduction can be achieved by externally rotating the hip to clear this bony landmark. Hip Internal or Medial Rotation - this occurs when the femur rotates on its own long axis and the toes of the foot move toward the middle of the body. The entire lower leg moves as a unit. Hip External or Lateral Rotation – this occurs when the femur rotates on its own long axis and the toes of the foot move away from the middle of the body. There are additional movements at the hip that can occur when the femur is fixed below and the pelvis moves from above. The pelvis can tip forward from its superior aspect into anteversion. This motion increases the arch or lumbar lordosis in the spine. The pelvis can tip backward from its superior aspect into retroversion which decreases the arch in the back or decreases lumbar lordosis. There is also some rotation or tipping of the pelvic ring over the legs as the body propels itself forward in space or shifts weight from leg to leg. Muscles Around the Hip Joint The Hip Flexors and Extensors Iliopsoas The primary hip flexor is the psoas, which has already been discussed. It has an intimate connection to the spine, the pelvis, and the lower extremity. If the iliacus is shortened it can pull the leg into a flexed position or pull the spine forward into a forward bent position. In a society in which individuals do a lot of sitting this is a concern, since the hip flexor remains in a shortened position for extended periods of time. If that muscle is chronically shortened it can cause movement restrictions and pain syndromes. When the muscle performs a shortening or isotonic contraction it will bring the femur or leg bone toward the trunk – ie hip flexion. Gluteus Maximus The antagonist or opposite muscle to the hip flexor is the large and powerful gluteus maximus. It is the large buttock muscle located posterior to the sacrum. It produces hip extension when activated. If the gluteus muscle is weak, the posterior support from below the pelvis can be compromised allowing more stress on the pelvis and lumbar spine. Other less powerful muscles may need to perform the hip extension motions and can result in problems in the pelvis and lower leg. Shortening of the gluteus can change the alignment of the pelvis and produce a slight anterior tip to the pelvis. Adduction and Abduction of the Hip The lower leg moves in several direction under the trunk and pelvis. Flexion and extension was mentioned