Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
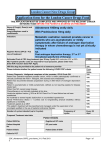
EVE3_ver3.0 National Cancer Drugs Fund Application Form – Everolimus for advanced renal cell carcinoma after previous treatment. Patient NHS No: Trust: Patient Hospital No: Practice Code: Patient's Initials and DoB: GP Postcode: Choose Consultant: Consultant Name: * Other Contact Details: Notification Email Address: * (@NHS.net account ONLY) Treatment Start Date: BY TICKING THESE BOXES AND SUBMITTING THE APPLICATION THE CLINICIAN IS CONFIRMING THE PATIENT MEETS ALL THE CRITERIA BELOW. IT SHOULD BE NOTED THAT THE SACT DATASET WILL BE USED TO MONITOR THAT THESE CRITERIA ARE BEING MET: Please indicate whether patient meets the following criteria: Please tick 1. I confirm that an application has been made by and the first cycle of systemic anti -cancer therapy will be prescribed by a consultant specialist specifically trained and accredited in the use of systemic anti-cancer therapy. Yes No Yes No Yes No Yes No 2. I confirm that the patient has biopsy proven renal cell carcinoma 3. I confirm that the patient has progressed during or after treatment with vascular endothelial growth factor targeted therapy 4. I confirm that the use of everolimus will be as per the Summary of Product Characteristics (SPC). 5. What is the acquisition cost of the drug including VAT (if applicable)? £ per month: Commissioners will complete if cost not known as this will allow us to ensure budgets are allocated appropriately.