Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Marburg virus disease wikipedia , lookup
Herpes simplex wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Herpes simplex virus wikipedia , lookup
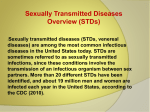
Oesophagostomum wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Diagnosis of HIV/AIDS wikipedia , lookup
Epidemiology of HIV/AIDS wikipedia , lookup
Epidemiology of syphilis wikipedia , lookup
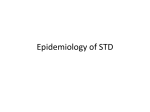
Microbicides for sexually transmitted diseases wikipedia , lookup
Common Sexually Transmitted Diseases (STDs) and HIV-Infected Women October 2007 This slide set was developed by members of the Cervical Cancer Screening Subgroup of the AETC Women's Health and Wellness Workgroup: Laura Armas, MD; Texas/Oklahoma AETC Kathy Hendricks, RN, MSN; François-Xavier Bagnoud Center Supriya Modey, MBBS, MPH; AETC National Resource Center Andrea Norberg, MS, RN; AETC National Resource Center Peter Oates, RN, MSN, ACRN, NP-C; François-Xavier Bagnoud Center Jamie Steiger, MPH; AETC National Resource Center Other subgroup members and contributors include: 2 Abigail Davis, MS, ANP, WHNP; Mountain Plains AETC Lori DeLorenzo, MSN, RN; Organizational Ideas Rebecca Fry, MSN, APN; François-Xavier Bagnoud Center Pamela Rothpletz-Puglia, EdD, RD; François-Xavier Bagnoud Center Jacki Witt, JD, MSN, WHNP; Clinical Training Center for Family Planning 2 Learning Objectives 1. Identify the five most common STDs affecting HIV-infected women 2. Discuss clinical presentations associated with the five common STDs 3. Recall methods for diagnosing the five common STDs 3 Common STDs in HIV-Infected Women 1. 2. 3. 4. 5. Herpes Simplex Virus (HSV) Syphilis Chlamydia Gonorrhea Trichomoniasis 4 Herpes Simplex Virus (HSV) 5 HSV: Clinical Presentation Primary Infection Recurrent Disease Prodrome phase: Tingling/itching of skin Appearance of painful vesicles in clusters on an erythematous base Vesicles ulcerate then crust over and heal within 7-14 days Viral shedding continues for up to 2-3 weeks After primary infection, virus migrates to sacral ganglion and lies dormant Reactivation occurs due to various triggers Reoccurrence is usually milder and shorter in duration 6 Herpes Simplex in Women with AIDS 7 Credit: Jean R. Anderson, MD HSV: Diagnosis Clinical presentation Viral culture Tzanck smear/Giemsa smear Skin biopsy 8 HSV: Treatment Considerations Antivirals Lesions may be bathed in mild soap and water Sitz baths may provide some relief Sex partners may benefit from evaluation and counseling Transmission is possible when lesions not present due to viral shedding 9 Syphilis 10 Syphilis: Clinical Presentation Primary / Infectious / Early Syphilis Stage: Primary Phase Primary chancre Begins as papule and erodes into painless ulcer with a hard edge and clean base Usually in the genital area Appears 9-90 days after exposure Can be solitary or multiple (eg. kissing lesions) Heals with scarring in 3-6 weeks and 75% of patients show no further symptoms 11 Primary Chancre Primary Chancre Credit: Centers for Disease Control and Prevention (CDC) 12 Syphilis: Clinical Presentation (continued) Primary / Infectious / Early Syphilis Stage: Secondary Phase Occurs 6 weeks – 6 months after chancre Lasts several weeks Accompanied with fever, malaise, generalized lymphadenopathy, and patchy alopecia Maculo-papular rash usually on palms and soles Condyloma lata on perianal or vulval areas Possible mild hepatosplenomegaly 13 Syphilitic Rash Credit: Dr. Gavin Hart and CDC Credit: Connie Celum and Walter Stamn and Seattle STD/HIV Prevention Training Center 14 Condyloma lata Condyloma lata 15 Credit: CDC Syphilis: Clinical Presentation (continued) Secondary / Latent Stage: Positive serology Rapid Plasma Reagin (RPR) Venereal Disease Research Lab (VDRL) Patients are asymptomatic and not infectious after first year, but may relapse One-third will convert to sero-negative status One-third will stay sero-positive but asymptomatic One-third will develop tertiary syphilis 16 Syphilis: Clinical Presentation (continued) Tertiary Stage: Cardiovascular: Aortic valve disease, aneurysms Neurological: Meningitis, encephalitis, tabes dorsalis, dementia Gumma formation: Deep cutaneous granulomatous pockets Orthopedic: Charcot’s joints, osteomyelitis Renal: Membranous Glomerulonephritis 17 Syphilis: Diagnosis Requires demonstration of: Organisms on microscopy using dark field Positive serology on blood or cerebrospinal fluid (CSF) Non-Specific Treponemal Tests: 1. Venereal Disease Research Laboratory (VDRL) 2. Rapid Plasma Reagin (RPR) 18 Syphilis: Diagnosis (continued) Positive serology on blood or CSF Specific Treponemal Test: 1. Fluorescent Treponemal Antibody Absorption (FTA-ABS) 2. Microhemagglutination-Treponema pallidum (MHA-TP) Organism may not be cultured but diagnosis cannot be determined by clinical findings only 19 Syphilis: Treatment Considerations Primary/ secondary/ latent stage: Benzathine penicillin Neurosyphilis: Penicillin G Ask about penicillin allergy before treatment Jarisch-Herxheimer reaction may occur 20 Chlamydia 21 Chlamydia: Clinical Presentation Mucopurulent cervicitis/vaginal discharge Dysuria Lower abdominal pain Urethritis, salpingitis, and proctitis Post coital bleeding – friable cervix Key Considerations: 50% of females are asymptomatic Sterile pyuria with urinary tract symptoms should trigger you to think chlamydia 22 Cervicitis Credit: University of Washington and Seattle STD/HIV Prevention Training Center 23 Chlamydia: Diagnosis Chlamydia culture New tests include: Direct immunofluorescence assays (DFA) Enzyme immunoassay (EIA) 24 Chlamydia: Treatment Considerations Antibiotics Azithromycin Evaluate and treat sexual partners Avoid sex for seven days after completion of treatment 25 Gonorrhea 26 N. gonorrhoeae-gram negative diplococci Diplococci 27 Credit: Negusse Ocbamichael and Seattle STD/HIV Prevention Training Center Gonorrhea: Clinical Presentation Areas of Infection Urethra Endocervix Upper genital tract Pharynx Rectum Signs and Symptoms Frequently asymptomatic Vaginal discharge Abnormal uterine bleeding Dysuria Mucopurulent cervicitis Lower abdominal pain 28 Gonorrhea: Diagnosis Clinical exam Cervical culture Polymerase chain reaction (PCR) or ligase chain reaction (LCR) Gram stain–polymorphonucleocytes with gram negative intracellular diplococci 29 Gonococcal Isolate Surveillance Project (GISP) — Percent of Neisseria gonorrhoeae isolates with resistance or intermediate resistance to ciprofloxacin, 1990–2005 Percent 12.0 Resistant Intermediate resistance 9.0 6.0 3.0 0.0 1990 91 92 93 94 95 96 97 98 99 2000 01 02 03 04 05 30 Gonorrhea: Treatment Considerations Intramuscular Ceftriaxone For pregnant women only: Ceftriaxone single dose but substitute Quinolones with Erythromycin Do not treat with Quinolones or Tetracyclines Evaluate and treat all sexual partners 31 Trichomoniasis 32 Trichomoniasis: Clinical Presentation Signs and symptoms: Vulvar irritation Dysuria Dyspareunia Pale yellow, malodorous - gray/green frothy discharge Strawberry cervix, inflamed and friable 33 Strawberry Cervix Credit: Claire E. Stevens and Seattle STD/HIV Prevention Training Center 34 Trichomoniasis: Diagnosis Flagellated, motile trichomonads on wet mount Vaginal pH > 4.5 Diagnosis confirmed by microscopy Other FDA approved tests: OSOM Trichomonas Rapid Test Affirm VP III 35 Trichomoniasis: Treatment Considerations For HIV-infected women: same treatment as non-HIV infected women Metronidazole or Tinidazole Sex partners have to be treated 36 Providing Culturally Competent Care The following factors can influence a woman’s understanding of STDs and need for screening: Language and literacy level Cultural and social background and its impact on her understanding of health, illness, and the female anatomy Comfort with discussing sexual health issues Comfort and previous experience with STD screening or testing History of sexual abuse and/or domestic violence may cause anxiety and exam refusal 37 Pearls of Wisdom Get comfortable with obtaining a thorough sexual history Check oral cavity if genital STD suspected Minimum of annual screening for STDs is recommended, with more frequent screening if high risk behaviors are reported Partner notification and risk reduction counseling for both patient and partner is an important part of treatment and follow-up. 38 Conclusion STD screening and treatment should be a primary intervention and a standard of care in all health care settings. Women infected with STDs have increased chances of contracting HIV. Studies show STD and HIV co-infection increases HIV virus shedding in the patients’ genital secretions. If co-infection is present, proper diagnosis and treatment of STDs will decrease the chances of transmitting HIV. 39 Helpful Resources AETC National Resource Center (NRC), www.aidsetc.org Clinical Manual for Management of the HIV-Infected Adult AIDSMAP,http://www.aidsmap.com Centers for Disease Control and Prevention, http://www.cdc.gov/std STD Treatment guidelines 2006 HIV / AIDS and STDs Health Resources and Services Administration HIV/AIDS Bureau, http://hab.hrsa.gov/ A Guide to the Clinical Care of Women with HIV/AIDS HIVInsite, http://hivinsite.ucsf.edu Transgender Awareness Training & Advocacy http://www.tgtrain.org/ 40 References Anderson, J.R, ed. (2005). A Guide to the Clinical Care of Women with HIV. Health Resources and Services Administration HIV/AIDS Bureau. Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines 2006. MMWR, Aug 4, 2006, 55. Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines 2006. MMWR, April 13, 2007, 56 Centers for Disease Control and Prevention. The Role of STD Detection and Treatment in HIV Prevention. Retrieved on September 16, 2007 from http://www.cdc.gov/std/hiv/STDFact-STD&HIV.htm#WhatIs Health Resources and Services Administation, HIV/AIDS Bureau, AETC National Resource Center. (2006). Guiding Principles for Cultural Competency. Retrieved on September 20, 2007 from http://www.aidsetc.org/doc/workgroups/cc-principles.doc US Preventive Services Task Force. Screening for gonorrhea: recommendation Statement. Ann Fam Med 2005;3:263-7. 41